
One of the components I love about this residency at Scottsdale Healthcare is the amount of information to which we are exposed. One of the core sets of readings we have includes the APTA Orthopaedic Section's Current Concepts for each joint, both standard and post-op. These readings give us some of the most up-to-date findings regarding ROM measurements, anatomy, special tests, examination and treatment techniques. What is really nice is that the authors of each section are typically the ones responsible for writing the questions on the OCS exam.
While the information from the Current Concepts readings is useful for treating each pathology, it unfortunately can stray away from a more important part of our plan of care. The Current Concepts readings (and much of what we were taught in PT school) function in that they identify the source of the pain and how to treat that specific structure and the pathologies associated with it. What they don't do is help us identify the cause of the of pain development in that structure. Another large chunk of our readings come from Sahrmann's Movement Impairment Syndromes books. She emphasizes the importance of assessing subtle joint movements. These are often the key to determining why a patient developed pain. Take a patient with groin pain with hip flexion. Our special testing may tell us that there is some femoral acetabular impingement, but WHY is that occurring? Reading the evidence alone will tell you it's because of bony deformities such as pincer and CAM lesions, but remember how bone deformities develop. Bone grows in response to stress. That means that often the CAM and pincer lesions only developed as a result of repeated contact as a result of abnormal joint mechanics (yes there are likely genetic bone deformities as well). By assessing the actual joint mechanics we can determine why that impingement ever started. Sahrmann teaches using palpation of the greater trochanter during hip flexion (or the affected motion) to determine the mechanics. If the greater trochanter glides anteriorly with hip flexion, it's no wonder the patient is experiencing impingement! Often this is a result of decreased strength of gluteus maximus and iliopsoas, along with the patient having a preference for recruitment of hamstrings for hip extension and a tight posterior capsule. Another example I have seen quite frequently since starting my residency has involved shoulder impingement. In school and in the literature, subacromial impingement is the primary type of impingement addressed. We are taught to utilize special tests and clusters to determine the diagnosis. Following accurate diagnosis, research gives us exercises that are commonly used for treating that diagnosis. What is the problem with this? Again we are ignoring why the patient developed impingement in the first place. Without understanding the cause, we may be incorrect with the type of impingement. Since covering this material in the residency, I have found far more cases of anterior glide/impingement compared to "subacromial impingement." Often your patients with the many types of impingement may test positive for your subacromial impingement clusters. This can be problematic if you are treating your patients based on diagnosis as opposed to an impairment-based approach. The types of impingement often require very different methods of intervention. If you are doing a thorough examination, you will find the accurate impairments and treat accordingly anyway! A lot of what Sahrmann teaches is common sense to the physical therapist upon retrospect. If we are thorough with our evaluation and treat the impairments (strengthen, mobilize, motor control training!), we would end up with the same result. Yet, Sahrmann's readings do an excellent job of bringing everything together and forcing us to actually live up to our name - movement specialists. It is easy to get lazy and not do a thorough movement analysis at the joint level. While special tests have their place (especially in the acute/traumatic cases), I am finding the use of them less and less important the more I work with an impairment and movement-driven approach. By going back to anatomy and fully assessing movement, we can determine why the structure ever developed pain in the first place and restore proper movement patterns. -Chris
5 Comments
 Learning, re-learning, challenged, fun. Those are the four words I would use to describe my experience in USC's sports residency program thus far. The experience has been absolutely incredible.
As football season comes to a close, what I have noticed the most is the experience I have gotten with acute injuries on the field. I'm comfortable being the first one to run on the field, assess the injuries, and make the appropriate decision. The thing about very acute injuries is often they do not present as they would in a clinical setting. This is why I think going through a sports residency is so crucial to developing skills as a sports physical therapist. Furthermore, for a player who complains of shoulder pain, its very hard to assess a dislocated shoulder with all the pads on. Learning new tricks to assess injuries with pads on was a really useful tool for me. More importantly, just being able to see these injuries have been tremendous to my growth as a sports PT. Concussions, ACL's, MCL's, hip pointers, broken tibia, ankle sprains, grade 1-3 AC joint sprains, dislocated shoulders, cramps, bone bruises, and many more. The USC literature reviews each week that both the sports and orthopedic residents come together to discuss have been very eye-opening. We come together with the orthopedic residency director to discuss the backgrounds of all the authors of the articles and the articles relevance/downfalls. This has really opened my eyes to how effective the practice guidelines are, the CPR's relevance, and much more. Always is good to have a critical eye when analyzing evidence. Finally, USC brought in Laurie Hartman and Bill O'Grady this past week for all the USC residents/faculty to discuss manipulations and have a lab. It was unbelievable to feel and see how these two pioneers performed manipulations! Lastly, the mentoring aspect of the program is what I have valued the most. In addition to getting the 4 hours of patient mentoring each week, I have been able to have additional mentoring on manual skills/special tests/interventions every Tuesday with two mentors. Each week we pick a body part and go through each test and different manual skills. They say practice makes perfect and I think this has been a really key component to my skills developing. Also, I have had unscheduled mentoring on multiple occasions. The best example of this was when I brought one of my college pitchers out to throw and one of mentors brought her MLB guys out to throw as well. My mentor spent time and helped me look at different throws to determine what to look for and what I should think about when fixing mechanics. It's times like those that I am really happy I chose USC's sports residency. I'm adding new techniques and reflecting on my clinical reasoning each week and have seen a marked improvement. -Brian  A big part of a residency program is the 1-on-1 mentoring that occurs each week. At the Harris Health System Orthopedic Residency, I am fortunate enough to get at least 5 hours of mentoring each week. In order to maximize the effectiveness of each session, the program faculty have drafted a form that residents are expected to complete prior to each mentor session. This forms gives both the resident and faculty mentor a clear picture of the patient they are about to treat. Key features include: Red Flags, Pertinent Positives and Negatives regarding patient status, literature to reinforce each intervention selected, and Asterisks signs.
The form is useful for anyone, especially those difficult patients where prioritizing interventions can be difficult. I recommend this form to any student or clinician who is trying to better organize their treatment session. Click the link below to access the form: /uploads/1/3/2/6/13261333/ortho_mentorship_form_for_tsptwebsite.pdf -Jim NSC was this past weekend and for those of you who may have missed it, here is the link to an interview with John Dewitt speaking on the topic of residencies/fellowships. Here he discusses what the difference is between the two, when you should consider participating in a residency, the financial concerns, and more.  One of the best things about USC's sports residency program is the ability to be flexible with schedules. These past few days, I had the opportunity to cover AVP's Professional Beach Volleyball tournament in Huntington Beach, CA. Now I'm not gonna lie, working on the beach was pretty awesome. However, it was the full experience that made it such an unbelievable learning environment. The event was being covered by full team of healthcare professionals: PT's, ATCs, DCs, MDs, MT's, and EMT's. WIth the diversity of the group, each athlete was ensured to get whatever treatment they needed. I covered the Thursday qualifying round and the Friday rounds. My duties included stretching, assessing, treating, and taping athletes. It had the luxury to have different professionals right next to me when I needed to refer out to them. What I really loved about this event was each sports medicine professional was there to teach each other something new. I learned different kinesio tape methods which was very helpful for me. Also, I was able to see how different healthcare professionals approached their treatment with the athletes. In addition to working the event, when there was down time in the medical tent we were allowed to cover the games and watch the games. It's amazing to see these athletes cover so much ground in a short amount of time. Many of these athletes are in amazing shape and would come in regularly before and following games to get soft tissue work even if they didn't have an injury. The one thing I took away from working this event, besides how much fun it was to work on professional athletes, was the amount of collaboration between all of the sports medicine professionals. We all were able to work efficiently and effectively together to help each athlete the best we could. It goes to show that a team of different sports medicine professionals can work together for the best treatments.
 A few of the faculty members at the Harris Health System Orthopedic Residency started a Manual Therapy Fellowship program, OPTIM PT, last year. Part of their fellowship is devoted to pain management and how to incorporate manual therapy in the treatment of chronic pain. To introduce the topic of pain management, they brought in Rod Henderson, physical therapist and specialist in pain management. As a bonus, they let the Orthopedic residents attend the course as well. During the course, we covered the physiology of pain, pain theories, how to educate, and select appropriate interventions. Let me be clear now, we are not just talking about chronic low back pain. Chronic pain is present in a significant number of musculoskeletal problems. Consider the knee replacement patient who has had pain and decreased quality of life for the past few years; or consider any type of tendinopathy patient. Both of these patients are in a chronic state of pain.
Before we begin talking about pain, it is important to accurately define the word. Pain can be defined as a sensory and emotional experience in response to actual or potential tissue damage. The pain response has both protective and adaptive abilities, and is a necessary and important part of our lives. While it is necessary, the transformation from acute to chronic pain is where it can become a problem. The dominating theory of pain science today is the Pain Neuromatrix, a theory that has not fully made it into physical therapy schools yet. In this theory, there is no true "Center of Pain." The Neuromatrix theory suggests that there are several factors (inputs) that determine a person's reaction to pain (output). Inputs include sensory, cognitive, and affective components that all interact with each other to determine how the person will perceive a stimuli, what actions need to be taken, and the appropriate stress regulations. The inputs are heavily determined by past experiences and the person's expectation to a certain situation. When you have chronic pain, there is an expansion of the receptive fields that send input to the brain. Certain stimuli will begin to have heightened states of sensitivity. This can manifest as pain with light touch, an increased heart rate, or sending the patient into tears. For example, a stimulus that previously went unnoticed, like putting on a pair of socks, can become immensely painful if your nerves are sending mass amounts of improper triggers to your brain. It is our task to rewire these inputs, using graded exercise, desensitization, and proper education. A few take home points to remember when treating any chronic pain patient: -All pain originates in the brain. I would suggest finding a tactful method to tell the patient that news. They probably will not come back if you simply say the pain is just in their head. -The amount they hurt does not equal the amount of tissue damage that is present. Think about a paper cut on your index finger. It is rather small, but it can hurt a whole lot. Many people with chronic pain have completely healed "paper cuts", but their brain is responding as if the event just happened. -Patients with chronic pain have maladaptive thoughts and beliefs. Many of these thoughts and beliefs go beyond their physical appearance. Most have additional stresses at work and home, complicating their musculoskeletal pains. Address these issues in your plan of care. -Chronic pain implies that the issue has been present for a long time. Do not expect to heal these people in 1 or 2 treatments. I know you did not go to PT school to become a psychotherapist, but other than psychologists we spend more time with our patients than any other healthcare provider. This is an unique advantage. Chronic pain is everywhere. If you are not learning how to incorporate the biopsychosocial model into your clinical practice now, you need to start. Understanding this will take your outcomes from good to great. -Jim  Well, I am about 2 months into my orthopaedic residency here at Scottsdale Healthcare and it has been quite an experience. Not only am I learning an incredible amount, but the area is beautiful as well. Starting off my first couple weeks, I was eased into the practice with a lighter caseload as I learned the ropes to documenting here. We started off our first day after orientation going through the EMR, so that we could find our way through the system. As helpful as it was, the best way to learn that sort of thing is to actually do it over and over again. The lower patient number each day initially was definitely beneficial while I was trying to become more efficient documenting. Once I had adapted to the EMR, my caseload was increased to that of the other physical therapists. We typically treat 1-on-1 with about 8 patients a day (depending on how many hours you work). I enjoy this individualized care so I can continually assess my patients and adjust any faults with their mechanics when performing exercises. It also allows more time for manual therapy if appropriate for that particular patient. As with any clinic, there can be fluctuating patient populations which may lead to "down time." Whenever I have no patient or paperwork to do, I'm able to observe one of the other clinicians. The benefit of being able to observe different PTs cannot be overstated. Everyone has their own "style" of care, so I can continuously become a little more rounded with my clinical reasoning.
Probably the thing that stood out to me the most thus far has been the mentoring. Each week, I get 4 - 8 hours of 1-on-1 mentoring with a clinician that has both OCS and FAAOMPT credentialing, along with dry needling certification. We work side by side when treating or evaluating patients and in our breaks discuss other patient cases. During PT school, I rarely had any patients that I found too difficult. Here, it seems like every other patient is extremely challenging or with atypical presentations. The ability to schedule these patients for my mentoring hours allows me to build upon my reasoning after working with my mentor and is definitely one of the highlights of residencies in my opinion. Another component of residencies is class work. Thus far, we have had 4 classes: residency overview/subjective interview, clinical reasoning/evidence-based practice, medical screening, and sacroiliac joint. The sacroiliac joint lecture was just this past week and is the first of all our lectures on the joints (we have lectures every other week). We have initial readings to do for each topic: the APTA monographs. These include readings on both non-surgical and surgical coverage of each joint based on the most recent evidence. The lectures then are created by our faculty and are followed up by lab, where we go over examination techniques, exercises, and extensive manual techniques. I feel like my PT school did a very good job covering the SIJ joint, but my confidence in treating and assessing the SIJ after that lecture and lab increased dramatically. The individual focus and conversational discussion of the material likely played a significant role. I am looking forward to covering the rest of the body. Some additional components of the residency that have begun include additional course work and case study presentation. Throughout the year I am required to present 3 interesting cases or cases where I implemented interesting techniques to my co-workers, along with the current evidence on the subject. Something that I have enjoyed particularly with this residency has been their appreciation of continuing education. As the hospital hosts some courses, we have the opportunity to attend for free. They are paying for my attendance at the AzPTA fall conference next weekend and have been extremely accommodating with allowing me to design my schedule so that I may attend other courses as well. I can't believe 2 months are already gone, but it should be a fun remaining 10 months! If you have any questions about the residency, feel free to ask. -Chris  Last week was the 2012/2013 Orthopedic and Neurologic Residency graduation at the Harris Health System. It was a great experience watching the current residents pass across the stage. Working with them for the past 2 weeks had been a good experience. It was impressive to see how far they had come as clinicians and educators in the field of physical therapy in just one year.
Another good aspect of being part of a reputable residency program is that they bring in a very distinguished keynote speaker. Our was Anthony Delitto. Delitto has done an incredible amount for the field of physical therapy, especially in the area of low back pain. For example he authored the Clinical Prediction Guideline on Low Back Pain. In addition to a keynote address, he gave a 2 hour con-ed lecture following the reception. The lecture focused more on his current initiative- how to reduce the overwhelming cost of low back pain. It was not your typical facts and stats that things need to change. He mentioned one statistic at the beginning: Low Back Pain costs Americans over $85 BILLION each year. This is the third greatest cost in all of healthcare, trumped only by heart disease and strokes. From there, he started talking about what he and his medical system in Pittsburgh, The University of Pittsburgh Medical Center (UPMC) are doing to decrease the costs associated with Low Back Pain. In its simplest form what they did was provide evidence based care. Amazing right? Well, the literature shows that only ~50% of PTs consistency use what is considered evidence based practice. Delitto and UPMC have created algorithms for low back pain that each PT must complete after an evaluation. The algorithm is essentially a checklist making sure you performed certain tests and obtained the necessary information. The algorithm also directed you toward a specific treatment classification in line with what is the highest evidence of care. He has also worked with hospital management and the insurance companies to create a bundling package, that ensures all patients considered for spinal surgery go to physical therapy prior to having surgery. This has significantly lowered costs as well. Bottom line: He challenged us to think about our current level of practice. Are we consistently using evidence based practice? I am sure your patients are getting better- so do mine- but are you doing it as quickly and efficiently as possible? To be consistently successful we must have a systematic approach to our treatment sessions.  My first month of the sports residency has already been an incredible experience that has produced beyond my initial expectations coming in. As a collective group, myself, Chris, and Jim thought we would give our followers an insight on our experiences thus far in separate posts.
Immediately following the board exam I began a 4 day intensive sports seminar course at one of USC's lab/residency classroom, the Movement Performance Institute. This course is also open to other therapists as a continuing education course. I was blown away by the quality of the education. Being my first course taught by USC instructors/alumni, it was a unique learning experience with a lot of hands on practicing. Additionally, I went through an 8 day orthopedic seminar also hosted by USC. I think I added more manual therapy evaluation and treatment techniques in those 8 days then I had in my entire PT clinical education. Clinic/On-Field Experience: Currently, I am working in the clinic 20-24 hours a week. My first week gave me the opportunity to work with a heavily sports based population. Something like 65% of my patients were sports related injuries, from weekend warriors to high schoolers to a few college athletes. I don't think I realized how many athletes came into the clinic. My time in the clinic is just part of it though. I am currently providing practice and game coverage at the high school and college levels which has been great. It is very busy and what I love most about it so far is that I am actually seeing real sports injuries. Clinicals only give you so much but to be able to feel that knee laxity with a valgus stress test and see a real sulcus sign for a recent dislocated shoulder is amazing. Furthermore, developing the skills to evaluate acute injuries on the sidelines though tape and pads is something that I believe will just make me that much more skilled as a sports clinician by the end of the residency. Taping/splinting, treating acute injuries, working with the athletic training staff, and performing pre participation physicals with sports medicine doctors sums up what my first month of the on-field experience has been. MD Rounds/Literature Reviews: Being able to do rounds with the Kerlan Jobe Sports Medicine Doctors has been pretty incredible. Besides the fact that these physicians are all the team doctors for the Lakers, Clippers, Kings, Angels, Dodgers, Mighty Ducks, LA Sparks, LMU, PGA, and Hollywood Park race tracks, they are truly invested in teaching. While I have only done 2 weeks of rounds thus far, I can already tell it is going to be an excellent learning experience. The literature reviews started this past week for me. It was mainly an introductory experience but we did do a lot of hands on practicing for the first review topic. Having the opportunity to review multiple articles on body parts and unique topics, debate them, and find ways to implement them is invaluable. Furthermore, each week we will practice all the techniques for those topics with critique from the other residents, as well as the USC orthopedic residency program director. Lastly, I participated in USC's white coat ceremony. Being that SLU implemented white coats after my class, it was very special to be a part of. USC's white coat ceremony inducted the DPT class of 2016, Residency class of 2013-2014, as well as the Residency graduating class of this year. USC brought in all of their PT faculty and some very well know alumni also. It was a great way to meet influential physical therapists and get their advice. Most of my days are filled from early mornings to late nights and while exhausting, it has been energizing. Many challenges are to come and I am looking forward to each and every one of them! Hopefully this will start to give you all an insight into what a sports residency is all about. Next up will be updates from Chris and Jim.
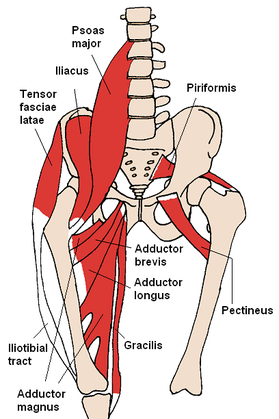
The iliopsoas is commonly regarded as a hip flexor, but it has two additional major functions: spinal compression and hip lateral rotation. The path of the muscle from origin to insertion begins on the lateral sides of the lumbar vertebral bodies, passes posterior to the vertebral column and then wraps posteriorly around the femur to the lesser trochanter. Acting as a spinal compressor, this muscle can be responsible for low back pain if short or stiff. Its role in lateral rotation can have a large impact on gait and jump mechanics as well. An individual that displays valgus knee positioning with squats often has weak hip abductors and lateral rotators. With the muscle wrapping around the femur posteriorly and acting as a lateral rotator, the iliopsoas is a muscle we definitely should consider in our intervention planning. This discussion lead me to realize the necessity of a 3-Dimensional understanding of our anatomy to further my knowledge in orthopaedics.
An example of anatomy's impact hit me with a patient in week 1. This patient presented with pretty clear signs/symptoms of a herniated disc. This patient described excruciating pain in her low back and hips after "trying to stretch her back and hamstrings out (this patient indicated she was doing so in a long-sitting method using primarily lumbar flexion)." She stated her pain is worsened by sitting and improved by standing/walking around. Pain increased and peripheralized with repeated lumbar flexion and centralized with extension. (+) SLR, Crossed SLR, and Slump Test. Following the evaluation, I prescribed prone press-ups, some core stabilization training exercises, and modification of lifting techniques. Stretching was deferred at this time as the patient was too acute and sensitive. At the follow-up visit a week later, the pain was mainly localized to the central spinal column, however her pain had switched from her posterior RLE to her L lateral thigh and inguinal area. This was somewhat an abnormal presentation to me, so I consulted my mentor. It turns out her distribution of her new symptoms were along the lateral cutaneous nerve at the lateral thigh, but also along the path of the nerve as it passes just inferior to the ASIS. The reason for the irritation lies in its lumbar innervation. This just happened to be an odd presentation as the pain switched extremities. So as you can see, it's not good enough to simply know what areas peripheral nerves and dermatomes contribute to and where the origins/insertions of muscles lie, but we must also strive to understand the path of the structures throughout the body. This will lead to improved clinical reasoning in both our examinations and interventions. -Chris |



 RSS Feed
RSS Feed