
|
|
|
RehabilitationAfter the diagnosis of an ankle fracture has been made, the region is typically immobilized with limited weight-bearing. The severity and location of the fracture contributes to the decision on what level of immobilization is required: open reduction internal fixation, CAM boot, aircast, etc... This timeframe for immobilization typically occurs for 4-8 weeks (factors like osteoporosis and peripheral vascular disease may impact the timeframe). Once radiographic evidence of sufficient healing occurs, the patient often begins skilled physical therapy. Initially, the primary focus will be on reducing swelling and improving joint mobility. This is often done with ROM and stretching exercises, joint mobilization, soft tissue treatment, and modalities. Open-kinetic chain strengthening exercises are typically started once the patient's fear of movement and activity tolerance improved. During this initial acute phase, gait training may be necessary to train the client on how to use crutches, how to maintain appropriate weight-bearing status, etc. As the patient gains mobility and weight-bearing is progressed (based on bone healing), weight-bearing exercises will be progressed. The patient may initially need to perform AAROM exercises in closed-kinetic chain in order to address any apprehension and improve load tolerance, while restoring mobility. Full ankle motion is not required nor expected before weight-bearing is initiated. Once the patient presents with sufficient tolerance, closed-kinetic chain load is progressed further with shuttle squats and calf raises, to full body versions as well. Exercise progression becomes more typical at this point as various methods of loading (lunges, squats, step-ups/downs, etc.). What likely needs to be addressed is stability training in some form to improve reaction and balance when stability is challenged. This can include standing on unstable surfaces, incorporating mental and upper extremity tasks, agility/plyometric training, etc.  This progression has no set time table. We have to respect the severity of the fracture, co-morbidities, prior level of function, planned activities to return to and more. Always consider the physician and/or surgeon's prescribed progression, but move your patient through the various phases based on how that specific individual is doing. A patient with a fibular fracture that also suffered a common peroneal nerve injury will likely not progress as quickly as the same fracture without neurovascular insult. There is no set timeframe for recovery from injury, so prepare to be flexible. You may need to incorporate other treatment methods to help move your patient through each step (spinal manipulation, nerve mobilization, therapeutic neuroscience education, among others). Regardless of the contributing factors, the therapists' objective is to guide the patient back to their prior level of function safely. -Dr. Chris Fox, PT, DPT, OCS Want to learn more advanced information to develop your clinical skills and knowledge? Check out the Insider Access Page!
1 Comment
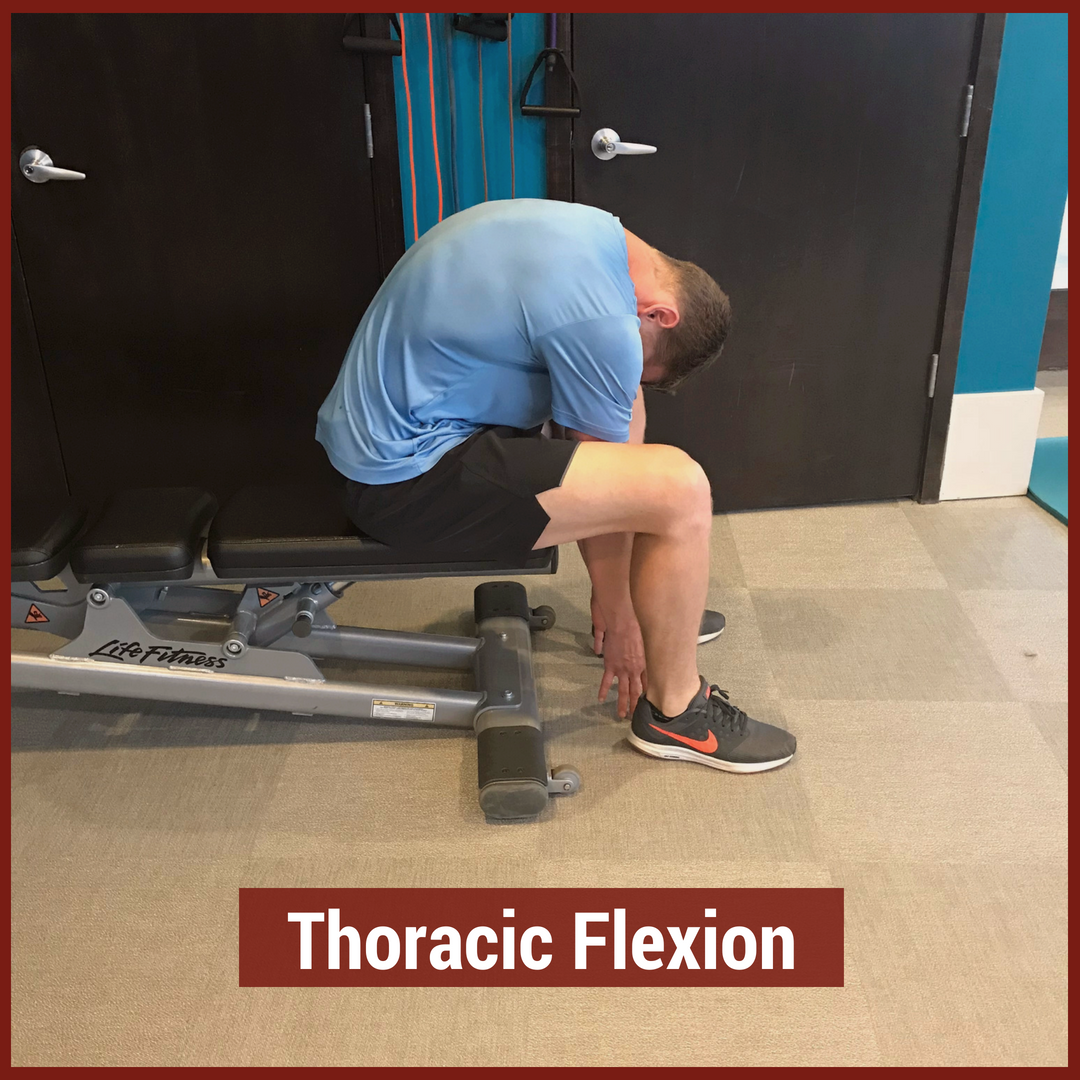
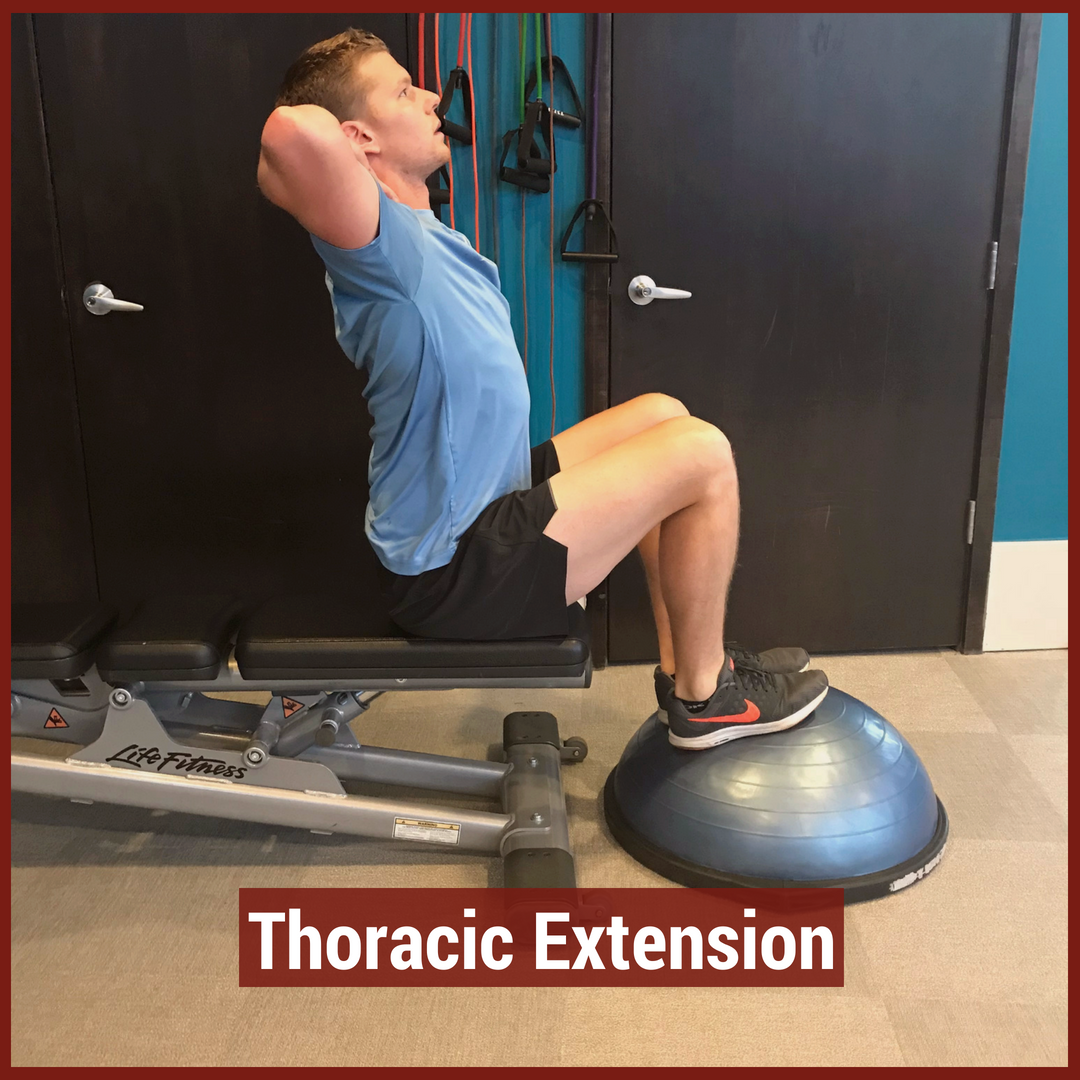
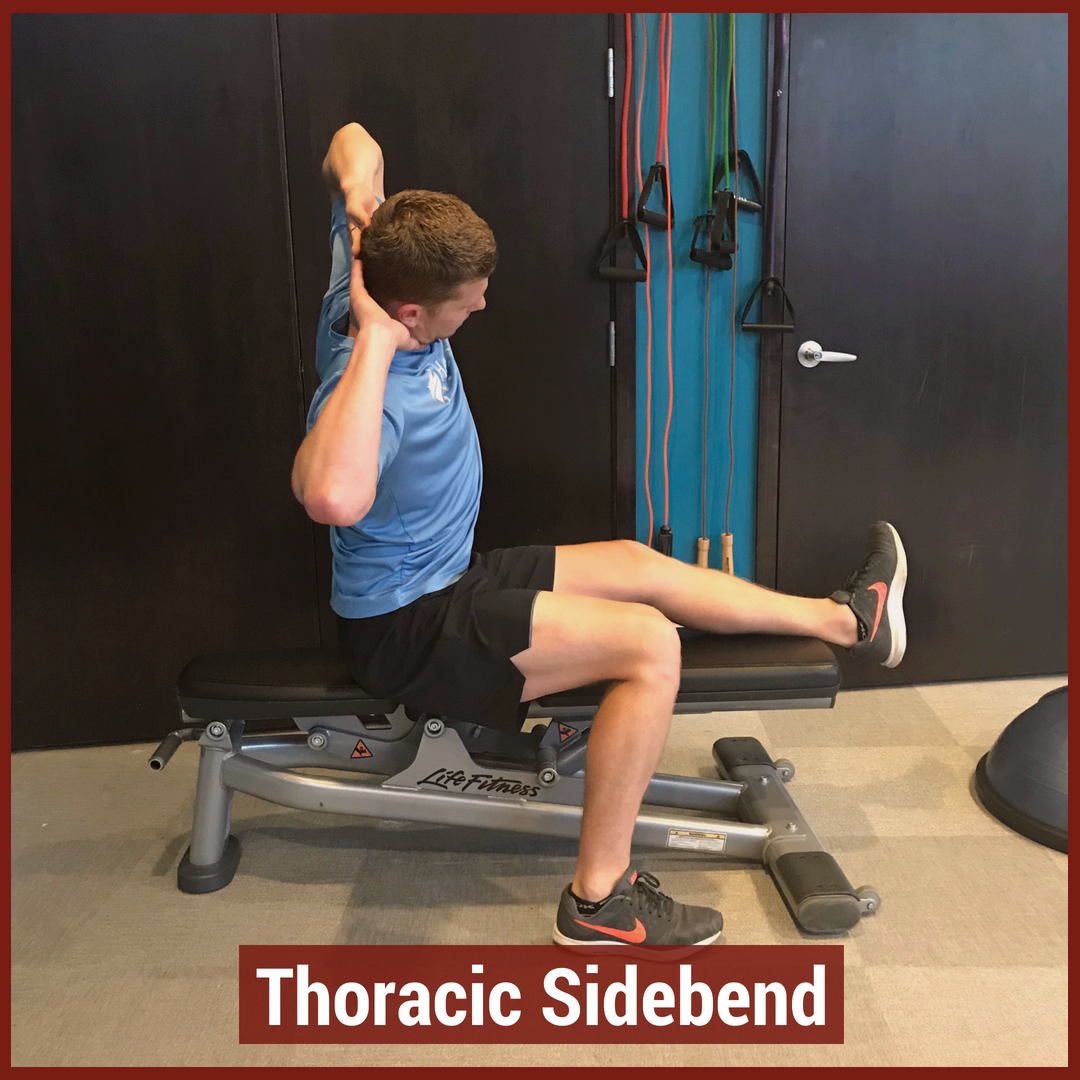
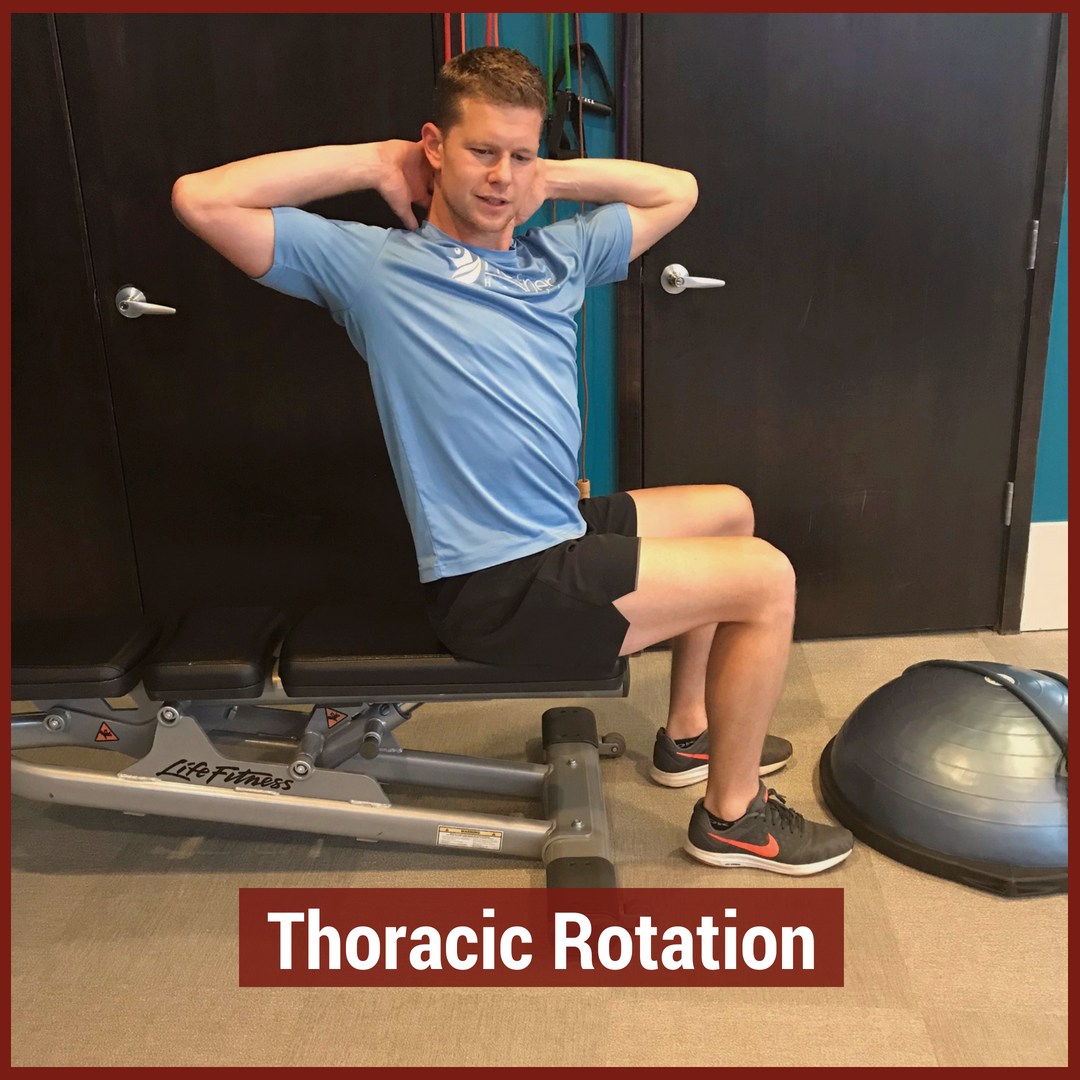
In physical therapy school, the thoracic spine is often glossed over during the musculoskeletal courses. This may be due to the low incidence and prevalence of thoracic spine pain. The incidence of thoracic spine pain is only ~15-19% across the population. This is relatively low compared to lumbar spine pain, which has an 80% prevalence in adults. Additionally, physical therapy schools may choose to emphasize the non-musculoskeletal diagnosis that are important in the thoracic spine. Since many organs are housed in the thoracic cavity, hours are spent on non-musculoskeletal diagnosis. For example, if a patient presents with thoracic spine pain, it is more important to rule-out a myocardial infarction than a thoracic facet restriction. Regardless, there is a gap in student's knowledge regarding thoracic spine anatomy and biomechanics, mobility assessment, and differential diagnosis. In this post, I will be reviewing the active range of motion and segmental mobility assessments for the thoracic spine. Additionally, I have added some clinical pearls for thoracic anatomy and biomechanics! Anatomy and Biomechanics Review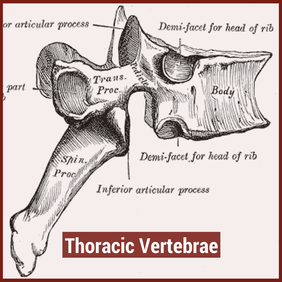 The thoracic spine is comprised of 12 vertebrae. These vertebrae have similar characteristics to cervical and lumbar spine- a vertebral body, pedicles directed posterior from the body, lamina that connect to form a spinous process, vertebral facets, and costal demi-facets (Neumann, 2010). The superior and inferior facets of the vertebrae are oriented ~60 degrees from the horizontal plane and ~20 degrees from the frontal plane. Since the thoracic spine connects cervical to lumbar, the junctional regions are important considerations as well. When transitioning from one region, there is no immediate change between cervical to thoracic vertebrae and thoracic to lumbar vertebrae. The superior thoracic vertebrae bare qualities similar to the cervical spine and the inferior thoracic vertebrae resemble the lumbar spine. This may explain why stiffness is often noted in these regions. 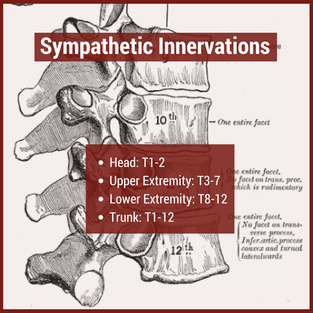 Additionally, the thoracic spine houses the sympathetic nervous system. The sympathetic nerve trunk lies anterior to the costotransverse joints. Clinically, this may help explain unusual symptoms that can be reproduced by neural tension tests such as the SLUMP TEST or Straight Leg Raise Test. Sympathetic innervations of the head arises from T1-T2, the upper extremities from T3-T7, the lower extremities from T8-T12 and the trunk from T1-T12. As Dr. Chris Fox wrote in a previous post on thoracic spine anatomy, "In the thoracic spine, T4-9 is known as the critical zone because the vertebral canal is narrowest here; it also has reduced blood supply (Egan et al, 2011). T6 is a tension point; here motion of the spinal core versus canal converge in different directions." Improving the neural mobility in the thoracic spine can help improve movement and decrease pain in the joints above and below. Active Motion AssessmentBelow are descriptions and pictures of thoracic spine active range of motion assessment. While it is impossible to isolate the thoracic spine, certain pelvis and lumbar spine positions can give the therapist a better idea of thoracic motion. In addition to the pictures below, I also assess thoracic flexion, extension, and rotation range of motion in quadruped.
Segmental Mobility AssessmentSegmental mobility is used to determine how much motion is available at each segment. In theory, this assessment is more specific than an active range of motion assessment as it tries to isolate each segment of the spine. While segmental mobility has been shown to have weak inter-rater reliability, practicing the assessment technique can be useful for improving tissue palpation and improving one's hands-on skills. Additionally, this assessment can help guide interventions when clustered with a patient's other symptoms.
Citations:
1. Briggs AM, Smith AJ, Straker LM, Bragge P. Thoracic spine pain in the general population: Prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskeletal Disorders. 2009;10:77. doi:10.1186/1471-2474-10-77. 2. Ganesan S, Acharya AS, Chauhan R, Acharya S. Prevalence and Risk Factors for Low Back Pain in 1,355 Young Adults: A Cross-Sectional Study. Asian Spine Journal. 2017;11(4):610-617. doi:10.4184/asj.2017.11.4.610. 3. Neumann, Donald. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 2nd edition. St. Louis, MO: Mosby Elsevier, 2010. 322-323. Print. 4. Egan W, Burns S, Flynn T, and Ojha H. The Thoracic Spine and Rib Cage: Physical Therapy Patient Management Utilizing Current Evidence. Current Concepts of Orthopaedic Physical Therapy, 3rd Ed. La Crosse, WI. 2011. Golf is a popular sport around the world, especially in our middle aged and older patients. Due to relatively low contact stresses, the sport is accessible for people of ranging physical capabilities. However, the biomechanics of the golf swing require proper mobility and stability throughout the body, especially at the shoulders, spine, and hips. Many of our wellness clients are golfers who simply want to perform at a higher level on the course. Most of the time, the missing link is unlocking the thoracic spine. Having proper mobility in the thoracic spine can improve the mechanics of the shoulders, low back, and hips. Biomechanical studies of the golf swing have shown a direct link between hip and shoulder rotation. From a structural standpoint, the thoracic spine is in the middle of those two joints and needs to be able to move. Additionally, the sympathetic nervous system is housed directly beneath the middle back, playing an important role in neural mobility. Many therapists prescribe tennis ball and foam rolling tricks for generalized t-spine mobility, but these are often isolated movements. For proper return to sport, therapists must be incorporating movements that engage the thoracic spine, while using the shoulders and hips. Furthermore, without t-spine rotation, the lumbar spine is required to produce more rotation. While lumbar rotation is not inherently bad, dispersing the rotational stresses throughout the spine is ideal. Using combined exercises for improving hip motion AND thoracic spine motion can useful for both rehab and warming up before golf. Below are a few effective treatment options to mobilize the thoracic spine. Spiderman'sTransverse Dowel T-Spine RotationStanding Stork TurnsStanding Step Thru's Exercises for Thoracic RotationHalf Kneeling Thoracic Spine Dowel RotationsInterested in more advanced content for your golfers? Check out our Insider Access!
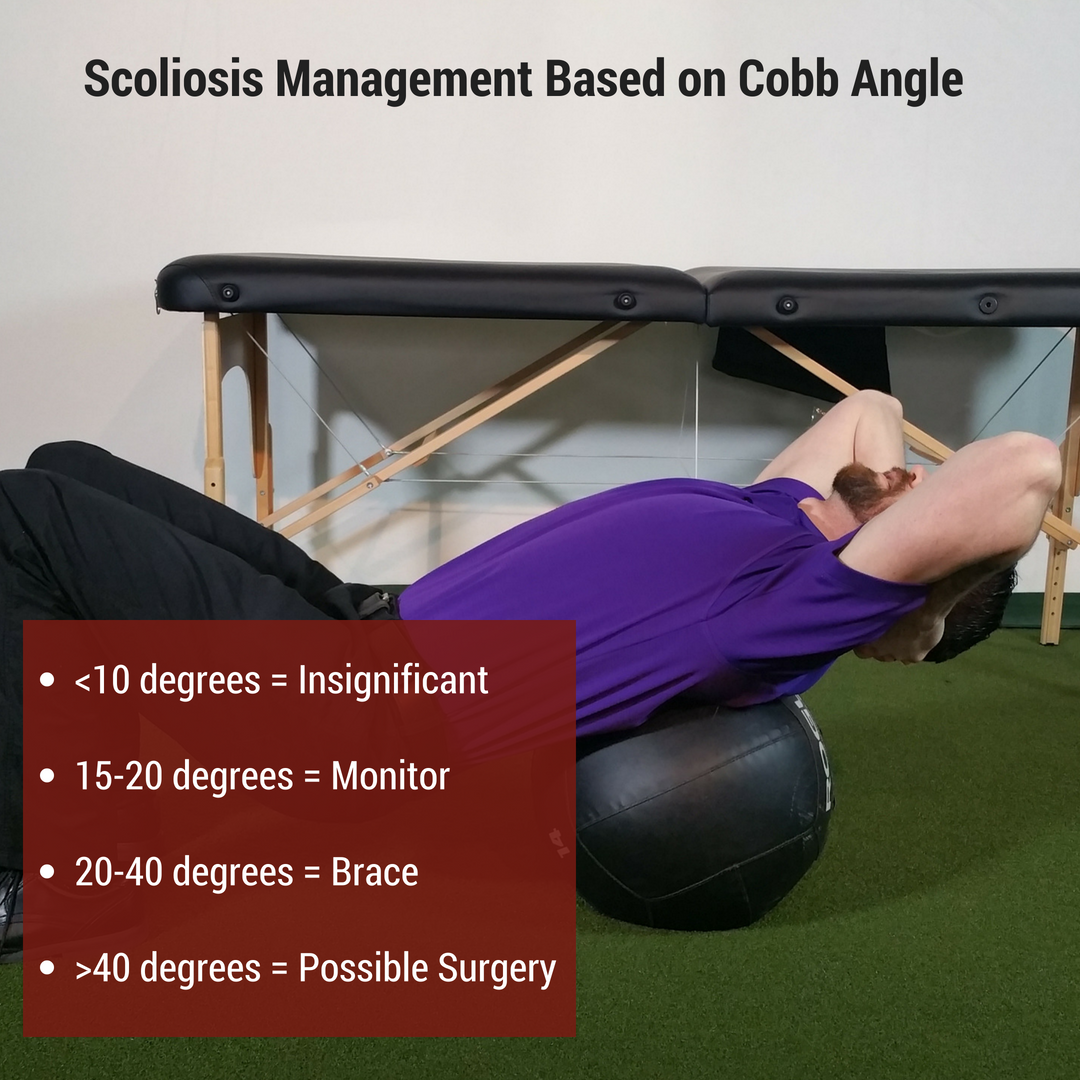
Dr. Brian Schwabe, PT, DPT, SCS, COMT, CSCS Scoliosis involves a 2- or 3-dimensional curve in the spine that can cause visual and/or functional abnormalities. It can involve curves that may go completely unnoticed in some and may impair lung function and daily activities in others. Scoliosis is a condition that has gone through a continuum of "best practice" treatments for decades. From requiring surgery to preventative bracing to minimal management, scoliosis continues to involve different severities of treatment. In PT school I remember learning I had scoliosis after learning how to perform the Adam's Forward Bend Test. I called my mother (a physician) after class to let her know, and she immediately started thinking I needed a consultation with an orthopaedic surgeon. Thankfully, my scoliosis is mild and I am past the developmental stage of life, so it hasn't required any specific management. Different Treatment Options for ScoliosisWhen the scoliosis is severe enough in an adolescent, either a Milwaukee Brace or TLSO (depending on curve location), can be used for treatment to prevent curve progression until the individual matures and the spine is less flexible; however, there are times when surgery is performed due to severity of curve or progression. Yet, when the curve is minimal, it is either ignored, "watched, " or sometimes physical therapy is prescribed (while some advocate exercises to correct imbalances associated with scoliosis, the research has not been shown to correct the asymmetry).
Emerging Research in ScoliosisThere are a variety of treatment methods for adolescents with scoliosis, but it is a condition that is managed later in life as well. While some surgeons will perform complex surgeries to correct/prevent progression of the curve, others choose to just monitor (similar to adolescents). However, with more imaging studies being performed, scoliosis appears to present as a possible normal asymptomatic spinal development in many individuals, in regards to its association with pain. Due to these developments, it is likely that a patient may be educated on pain and its lack of correlation with imaging findings. A 2018 article on idiopathic scoliosis found a link between thoracic scoliosis and lung function. In the study, thoracic scoliosis and hypokyphosis was correlated with decreased lung function. This is worth noting due to the importance of normal oxygen levels and proper function of the majority of systems in our body. For example, abnormal lung function may lead to cardiovascular disease. While the study had some faults in design, it should still get us thinking about if we should consider managing scoliosis differently. The first step would be to develop some additional research to determine the validity and strength of the correlation between scoliosis and lung function (and possibly cardiovascular disease later in life). Should the correlation be validated, indications for bracing/surgical/PT implementation would have to be developed. This may be based off measures like pulmonary function tests, Cobb angles, or other findings that can help with decision making on treatment strategies. Regardless, there is still a lot to be done in research regarding scoliosis, lung function, and its impact on mortality, but it may have more significance than we associate with many imaging findings these days. -Dr. Chris Fox, PT, DPT, OCS Reference: Farrell J1, Garrido E2. Effect of idiopathic thoracic scoliosis on the tracheobronchial tree. BMJ Open Respir Res. 2018 Mar 25;5(1):e000264. Want to learn more advanced information to develop your clinical skills and knowledge? Check out the Insider Access Page! In March 2016, I opened Heafner Health, a cash based physical therapy clinic in Boulder, Colorado. In the past two years, I have grown the business to consistently seeing 30-35 patients each week. While it has been an amazing journey, the past two years have taught me many lessons about business, physical therapy, and life. In the video below, Dr. Nick Helton PT, DPT and I chat about cash-based physical therapy. Nick is looking to transition from his physician owned outpatient orthopedic setting into a cash based clinic. In the video, we cover four main topic areas (these were taken from email communication between Nick and I):
If you have questions for Nick or myself OR would like a second round, please let me know in the comments section below.
Thank you for following TSPT, Jim Heafner PT, DPT, OCS Link to cash based practice website: www.heafnerhealth.com Have you ever seen or had a patient that has been doing exercises (maybe even ones that you've prescribed) for some specific muscles, but they continue to test weak, despite weeks or months of doing the exercises? It doesn't make sense. A weak muscle should respond to exercise right? What should you do at this point? There are 3 possible answers that I want to go over, in no specific order.  First, and perhaps most obvious, the patient may not be loading or performing the exercise properly. For example, if the patient is performing a clamshell, but instead of hip ER, they are rotating their spine, the muscle isn't being properly stimulated. That doesn't mean that there isn't still a benefit to the exercise, but it may not develop strength properly. In regards to loading, if a patient can perform an exercise for 20 or 30 repetitions, they may improve muscle endurance or neural activity, but it's unlikely strength changes will occur. One of our first steps with exercise prescription should be ensuring proper technique and appropriate dosage. Second, the muscle may not be improving in strength due to neural inhibition. If there is insufficient neural input, the muscle will have difficulty fully firing, despite the load that is put on the muscle. For example, if the femoral nerve has decreased nerve conduction due to restricted lumbar mobility, the quadriceps may not improve strength even with hundreds of squats. With these patients, our goal should be to improve the neural mobility at each point of restriction. At that point, the muscle may test completely strong without ever having done one strengthening exercise. An example of this is when a patient with weak L5 myotomes tests completely strong simply with some sideglides or press-ups. Finally, a patient may not progress in strength due to non-musculoskeletal issues. Issues can include conditions like multiple sclerosis, fracture, tumor, etc. But biopsychosocial factors can absolutely contribute as well. With how powerful the mind is, there may be some individual factors that are blocking any potential strength improvements. More medical conditions obviously warrant further testing and referral to the appropriate practitioners, but the biopsychosocial factors can be addressed by us as physical therapists.  So how do we handle the next patient that comes in with weakness not responding to exercise? I recommend first checking the form for the exercise and how the dosage has been. Should those be correct, assess for any nerve or mobility restrictions that may be causing neurogenic inhibition. Address those restrictions and re-check the strength deficit. You should be able to see some change relatively quickly. If the patient fails to respond to those techniques, do some additional fracture, UMN lesion, cancer, etc. screening and refer out, depending on the results. -Dr. Chris Fox, PT, DPT, OCS Do You Struggle Applying the Principles of Pain Science? Over the past several decades, pain scientists and researchers have made great progress in understanding and explaining pain. Unfortunately, even when the biology of pain appears to be simple, the answer is never straightforward. Each human being has their own set of experiences which impacts how they perceive pain. Science has shown us that using a biopsychosocial approach is integral in addressing these factors. This includes identifying one's biological, psychological, and sociological aspects that may be contributing to their pain. While this sounds great on the surface, it can be hard to apply these principles with each patient. The Basics of Teaching about the Science of Pain From my personal experiences, I cannot stress the importance of building a therapeutic alliance with the patient. As health and wellness providers, the ability to understand someone’s needs and tailor one’s language toward these needs will significantly influence the outcome of their situation. Building a strong therapeutic alliance is first and foremost! After a therapeutic alliance has been created, then the multiple factors that impact someone's pain can be explored. Three main areas I address are mindfulness, nutrition, and sleep (with the primary one being mindfulness). Each of these areas play an important role in the sensitivity of the nervous system. Addressing these factors can reduce the sensitivity in the body’s alarm system to foster an environment of healing. Strategies I Use to Implement Mindfulness 1) Manual Therapy: During manual therapy, I ask the question, "what do you feel?" This question brings awareness and perception to the patient's body part. It forces them to describe their current environment and take ownership over the symptoms they are experiencing. 2) Keeping a Journal of Symptoms: Journaling allows the patient to describe their situation and environment. It brings context around time, location, and external factors that may be influencing pain. With each journal entry, patterns will be identified that can help alleviate the onset of pain. 3) Meditation as Mindfulness. Identifying strategies to calm down the nervous system is beneficial. While this may seem to foreign for most people, meditation can be great for activating the parasympathetic nervous system- slowing down the heart rate and allowing the body to rest. It is simply not enough to tell a patient to be more mindful OR watch what they eat! As a profession, we must do a better job providing solutions and offering resources to assist with the multiple factors of pain.
-Jim Heafner PT, DPT, OCS A couple weeks ago, a video was discussed on some forums about allowing lumbar flexion during deadlifts. While I believe people have always had some lumbar flexion during deadlifts and squats, traditionally, many believe a "neutral spine" is required to safely load the spine during the movement. Recently, there has been an increase in education and awareness of the flexion motion of the lumbar spine during deadlifts and squats in order to help prove the normalcy of the movement pattern. It is in conjunction with the development and understanding of pain science research that we are learning how little abnormal movement patterns may matter. Does this mean we should change our complete philosophy of movements with strength training?
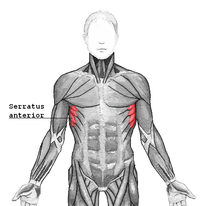
A couple years ago, I wrote a blog about changing scapular positioning during pressing motions. Many recommend performing a bench press with scapulae adducted in order to improve stability and open subacromial space. I proposed that we should consider altering the positions by adding protraction at the end of the bench press and shrug at the end of the military press in order to fully apply the strengthening exercise to the motions of the muscle fibers. The serratus anterior and pectoralis muscles have the function of protraction (SA also upwardly rotates the scapula). Why should we ignore that component of the muscle's function? There was some significant rebuttal from some clinicians out there on the basis of potentially damaging the rotator cuff by decreasing subacromial space. However, with the development of research showing the lack of correlation between pain and pathoanatomical findings, any "damage" that might be done with this movement pattern (if it actually occurs) can be deemed insignificant. Now, I am not suggesting that you immediately start training these alternative movement patterns with the load you typically use for your usual exercises. A new motion requires a new start. You will likely have to use significantly less weight when doing your first Jefferson curl compared to a typical deadlift. The same applies to the military press when you add a shrug at the top of the motion. Initially you will be weaker with these motions, but by training them, you will improve your strength and stability for positions that some might label as "unsafe" or "faulty." The real question that should come from these finding is should we decreasing our focus on research that emphasizes the biomechanical approach? If a RTC tear is not correlated with pain or possibly strength, why should we worry about how RTC tears develop? If a herniated disc doesn't correlate with pain or weakness, should we bother looking at studies focused on disc pressure? Personally, I believe we should still consider these concepts to some degree. Some disc herniations are significant enough to cause urinary retention. Arthritis may be significant enough to severely limit motion in a joint, decreasing the function of that joint. I am not saying that we should worry about every pathoanatomical finding either. I believe that there is possibly a middle ground to be met where pathology should still be considered, but shouldn't be the guiding force. I do not have the answer, but hopefully the research WILL continue in the mechanical area. Dr. Chris Fox, PT, DPT, OCS  Yes, I said it. I train knee valgus. But hear me out before you jump to conclusions. Instead, watch a basketball game. Look at a basketball player grabbing a rebound or taking a shot. If I'm a betting man I say you will see valgus at least 10 times a game. Yes, valgus can be bad, but it doesn't mean it shouldn't be trained to control it. Let's say you get a referral for a goalie who just had ACL reconstruction. How many of you would say you wouldn't train your goalie for return to sport activities? Well, part of that return to sport is training the goalie to get back to what they do best. Sometimes that means they prefer the "butterfly" position. In case you haven't seen what this looks like, its complete valgus. Yet, this is functional for their position. So do we train valgus in the basketball athlete and the hockey goalie? In my opinion, we need to help them learn how to control those positions. If the glutes help externally rotate the femur that means it slows down internal rotation. Why not eccentrically train these muscles and also get the athlete into a "safe" position to learn how to control it toward the terminal phase of rehab? if they are going to do it anyway, then we should be helping them control the position to minimize the risk of injury.  Dr. Brian Schwabe, PT, DPT, SCS, COMT, CSCS Board Certified Sports Physical Therapist LEARN HOW TO TRAIN SPECIFIC SPORTS & POSITIONS FOR RETURN TO SPORT WITH INSIDER ACCESS  The April 2018 National Physical Therapy Examination is quickly approaching. Since >50% of the examination covers musculoskeletal and neuromuscular content, it is important to spend ample time reviewing Orthopedic evaluation and examination. A portion of the Orthopedic examination is the special tests. While many of these special tests do not demonstrate good reliability individually, the diagnostic accuracy improves when clustered together. In this post, I outline the top 5 most important tests to know for the NPTE. NPTE Studying PostsImportant Special Tests for NPTE5. Lachman TestImportance of Test: The anterior cruciate ligament stabilizes against anterior translation of the tibia on the femur, due to the attachment at the anterior tibial plateau and posteriorly on the medial side of the lateral femoral condyle (Neumann 534). The force applied by the examiner stresses the ligament, and is a better test for assessing the integrity of the ACL in acute injuries compared to the Anterior Drawer Test for various reasons. The position of 20 degrees of knee flexion is a less painful position than the 90 degrees required for the Anterior Drawer Test; thus, there is a lower chance of protective spasms from the hamstrings. Also, in 20 degrees of flexion, the ACL is more maximally stressed and can be assessed more accurately, because other tissues due not limit anterior translation of the tibia ("Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis"). It should be noted that patients with a torn PCL may test positive with a Lachman test. In the starting position of the Lachman test, the tibia will rest further posterior than usual due to the absence of the PCL, leading to increased excursion during the test (Manske, 2006). This means PCL integrity should be assessed prior to looking at ACL integrity. Often with ACL injuries, other tissues and structures can be injured as well. One of the more significant findings recently has been bone contusions with ACL injuries. Look for research on the topic coming out soon! 4. Full Thickness Rotator Cuff ClusterSimilar to the hawkins-kennedy test for impingement, it is again important to cluster this test’s results with other tests and measures when assessing for rotator cuff tears. The cluster for a full thickness rotator cuff tear includes 1. the Drop-arm sign, 2. the painful arc sign, and 3. infraspinatus manual muscle test. If all three tests are positive, the +LR is 15.6. (Note is 3/3 are positive and the patient is greater than 60 years old the +LR increases to 28) If all three tests are negative the -LR is .16 If ⅔ tests are positive the +LR is 3.6 Note: Two of the three tests for this cluster are the same as the impingement syndrome cluster. The differentiating factor between impingement and rotator cuff tear is the drop arm sign for full thickness rotator cuff tears and hawkins-kennedy for subacromial impingement.  3. SLUMP TestImportance of Test: This test's results can be interpreted in multiple ways. Like other neural tension tests, the test may indicate if a patient is experiencing symptoms related to nerves adhering to various tissues while travelling throughout the body. The patient may experience stretching, pain, or other neurological sensation in the area of adhesions. Another use for the test is detecting lumbar disc herniations. With the flexed lumbar spine and hip completed simultaneously with the extended LE, the sciatic nerve and its respective nerve roots are put on tension to detect the potential of a disc herniation. The results of the test should be interpreted based on the patient's pain/symptoms for which they are seeking treatment. Looking for a more efficient way to incorporate the special tests into your examination? Check out Dr. Heafner's Guide to Efficient PT Examination. 2. Vertebral Artery TestImportance of Test: If a patient tests positive on the Vertebral Artery test, they may have Vertebrobasilar Insufficiency (VBI), but if they test negative on it, you CANNOT rule out Vertebrobasilar Insufficiency. The theory behind this test is to maximally stress the opposite vertebral artery by stretching it to decrease the space in the lumen of the artery. The position of extension with contralateral rotation has been shown to decrease the diameter of the artery, but, again, the diagnostic accuracy of the test is still poor. 1. Transverse Ligament TestImportance of Test: Whenever a you encounter a patient that has neck pain as a result of trauma or cervical instability, you should always inspect the integrity of the transverse ligament before any other exam measures. The transverse ligament is responsible for keeping the anterior facet of the atlas against the dens of the axis. It attaches on the medial side of each large, lateral process of the atlas with the anterior side of the middle part touching the odontoid process. This creates a wide space in the vertebral canal for the spinal cord to pass through, posteriorly. When the transverse ligament is damaged, the atlas can slide forward on the dens, decreasing the size of the vertebral canal for the spinal cord to go through. This can result in neurological symptoms, such as pain, weakness, a lump in the throat, etc. In this compromised position, any movements can impinge upon the spinal cord and cause potentially irreversible damage. The supine transverse ligament stress test works to reproduce symptoms in an instability patient, because the test works to decrease the space of the vertebral canal by pushing the atlas anterior on the axis. This motion is normally blocked by the transverse ligament. The Sharp-Purser test should be performed before the Transverse Ligament Stress Test, because the Sharp-Purser test works to reduce symptoms, while the Transverse Ligament Stress Test works to reproduce symptoms. (“Clinical Testing for the Craniovertebral Hypermobility Syndrome”). Any Tests We Missed?Add them to the comment section below and tell us why!
-Jim Heafner PT, DPT, OCS |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|



 RSS Feed
RSS Feed