
- Home
- About Us
- TSPT Academy
- Online Courses
-
Resources
- Newsletter
- Business Minded Sports Physio Podcast
- Day in the Life of a Sports PT
- Residency Corner
-
Special Tests
>
-
Cervical Spine
>
- Alar Ligament Test
- Bakody's Sign
- Cervical Distraction Test
- Cervical Rotation Lateral Flexion Test
- Craniocervical Flexion Test (CCFT)
- Deep Neck Flexor Endurance Test
- Posterior-Anterior Segmental Mobility
- Segmental Mobility
- Sharp-Purser Test
- Spurling's Maneuver
- Transverse Ligament Test
- ULNT - Median
- ULNT - Radial
- ULNT - Ulnar
- Vertebral Artery Test
- Thoracic Spine >
-
Lumbar Spine/Sacroiliac Joint
>
- Active Sit-Up Test
- Alternate Gillet Test
- Crossed Straight Leg Raise Test
- Extensor Endurance Test
- FABER Test
- Fortin's Sign
- Gaenslen Test
- Gillet Test
- Gower's Sign
- Lumbar Quadrant Test
- POSH Test
- Posteroanterior Mobility
- Prone Knee Bend Test
- Prone Instability Test
- Resisted Abduction Test
- Sacral Clearing Test
- Seated Forward Flexion Test
- SIJ Compression/Distraction Test
- Slump Test
- Sphinx Test
- Spine Rotators & Multifidus Test
- Squish Test
- Standing Forward Flexion Test
- Straight Leg Raise Test
- Supine to Long Sit Test
-
Shoulder
>
- Active Compression Test
- Anterior Apprehension
- Biceps Load Test II
- Drop Arm Sign
- External Rotation Lag Sign
- Hawkins-Kennedy Impingement Sign
- Horizontal Adduction Test
- Internal Rotation Lag Sign
- Jobe Test
- Ludington's Test
- Neer Test
- Painful Arc Sign
- Pronated Load Test
- Resisted Supination External Rotation Test
- Speed's Test
- Posterior Apprehension
- Sulcus Sign
- Thoracic Outlet Tests >
- Yergason's Test
- Elbow >
- Wrist/Hand >
- Hip >
- Knee >
- Foot/Ankle >
-
Cervical Spine
>
- I want Financial Freedom
- I want Professional Growth
- I want Clinical Mastery
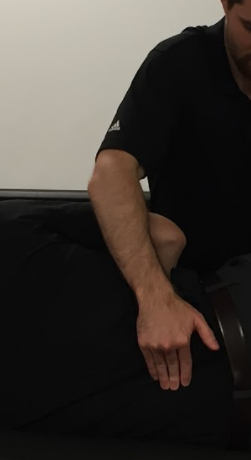

Phalen's Test
Purpose: To assess for carpal tunnel syndrome (CTS).
Test Position: Sitting or standing.
Performing the Test: The examiner passively flexed the patient's wrist maximally (but not overpressure), while maintaining the shoulder in neutral and elbow in extension. This position is held for 60 seconds or until symptoms are reproduced. A positive test occurs with numbness and tingling on the palmar aspect of the 1st, 2nd, 3rd, and radial half of the 4th digit within 60 seconds of assuming the position. The examiner documents the time at which symptoms were produced.
Diagnostic Accuracy: Extremely variable. Sensitivity: .10-.91; Specificity: .33-.86 (See articles listed in reference section).
Importance of Test: According to Neumann, the carpal tunnel is formed by the palmar surface of the carpal bones (scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, hamate) and the transverse carpal ligament. The transverse carpal ligament attaches to the pisiform and hook of the hamate on the ulnar side and the tubercles of the trapezium and scaphoid on the radial side. These borders create the carpal tunnel through which the tendons of the flexor digitorum profundus, flexor digitorum superficialis, flexor pollicis longus and median nerve travel. This is not a wide space at all. When pressure is increased in this area, people typically feel numbness and tingling on the palmar side of the thumb, 2nd, 3rd, and radial half of the 4th digit. Note: symptoms felt in the palm of the hand indicate pathology proximal to the carpal tunnel. The position of wrist flexion compresses the median nerve between the transverse carpal ligament and flexor tendons, producing neural symptoms. If overpressed, symptoms can be produced in healthy individuals as well.
Note: these tests should only be performed by properly trained health care practitioners.
Test Position: Sitting or standing.
Performing the Test: The examiner passively flexed the patient's wrist maximally (but not overpressure), while maintaining the shoulder in neutral and elbow in extension. This position is held for 60 seconds or until symptoms are reproduced. A positive test occurs with numbness and tingling on the palmar aspect of the 1st, 2nd, 3rd, and radial half of the 4th digit within 60 seconds of assuming the position. The examiner documents the time at which symptoms were produced.
Diagnostic Accuracy: Extremely variable. Sensitivity: .10-.91; Specificity: .33-.86 (See articles listed in reference section).
Importance of Test: According to Neumann, the carpal tunnel is formed by the palmar surface of the carpal bones (scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, hamate) and the transverse carpal ligament. The transverse carpal ligament attaches to the pisiform and hook of the hamate on the ulnar side and the tubercles of the trapezium and scaphoid on the radial side. These borders create the carpal tunnel through which the tendons of the flexor digitorum profundus, flexor digitorum superficialis, flexor pollicis longus and median nerve travel. This is not a wide space at all. When pressure is increased in this area, people typically feel numbness and tingling on the palmar side of the thumb, 2nd, 3rd, and radial half of the 4th digit. Note: symptoms felt in the palm of the hand indicate pathology proximal to the carpal tunnel. The position of wrist flexion compresses the median nerve between the transverse carpal ligament and flexor tendons, producing neural symptoms. If overpressed, symptoms can be produced in healthy individuals as well.
Note: these tests should only be performed by properly trained health care practitioners.
References:
Golding DN, Rose DM, Selvarajah K. "Clinical tests for carpal tunnel syndrome: an evaluation." Br J Rheumatol 1986 November; 25(4): 388-390.
Heller L, Ring H, Costeff H, Solzi P. "Evaluation of Tinel's and Phalen's signs in diagnosis of the carpal tunnel syndome." Eur Neurol 1986; 25(1): 40-42.
Katz JN,Larson MG, Sabra A et al. "The carpal tunnel syndrome: diagnostic utility of the history and physical examination findings." Ann Intern Med 1990 March 1; 112(5): 321-327.
D'Arcy CA, McGee S. "The rational clinical examination. Does this patient have carpal tunnel syndrome?" JAMA 2000 June 21; 283(23): 3110-3117.
Buch-Jaeger N, Foucher G. Correlation of clinical signs with nerve condution tests in the diagnosis of carpal tunnel syndrome." J Hand Surg Br 1994 December; 19(6): 720-724.
Gerr F, Letz R, Harris-Abbott D, Hopkins LC. Sensitivity and specificity of vibrometry for detection of carpal tunnel syndrome." J Occup Environ Med 1995 September; 37(9): 1108-1115.
Kuhlman KA, Hennessey WJ. "Sensitivity and specificity of carpal tunnel syndrome signs." Am J Phys Med Rehabil 1997 November; 76(6): 451-457.
Burke DT, Burke MA, Bell R, Stewart GW, Mehdi RS, Kim HJ. "Subjective swelling: a new sign for carpal tunnel syndrome." Am J Phys Med Rehabil 1999 November; 78(6): 504-508.
De SL, Steenwerckx A, Van den BG, Cnudde P, Fabry G. "Value of clinical provocative tests in carpal tunnel syndrome." Acta Orthop Belg 1995; 61(3): 177-182.
Neumann, Donald. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 2nd edition. St. Louis, MO: Mosby Elsevier, 2010. 219. Print.
Golding DN, Rose DM, Selvarajah K. "Clinical tests for carpal tunnel syndrome: an evaluation." Br J Rheumatol 1986 November; 25(4): 388-390.
Heller L, Ring H, Costeff H, Solzi P. "Evaluation of Tinel's and Phalen's signs in diagnosis of the carpal tunnel syndome." Eur Neurol 1986; 25(1): 40-42.
Katz JN,Larson MG, Sabra A et al. "The carpal tunnel syndrome: diagnostic utility of the history and physical examination findings." Ann Intern Med 1990 March 1; 112(5): 321-327.
D'Arcy CA, McGee S. "The rational clinical examination. Does this patient have carpal tunnel syndrome?" JAMA 2000 June 21; 283(23): 3110-3117.
Buch-Jaeger N, Foucher G. Correlation of clinical signs with nerve condution tests in the diagnosis of carpal tunnel syndrome." J Hand Surg Br 1994 December; 19(6): 720-724.
Gerr F, Letz R, Harris-Abbott D, Hopkins LC. Sensitivity and specificity of vibrometry for detection of carpal tunnel syndrome." J Occup Environ Med 1995 September; 37(9): 1108-1115.
Kuhlman KA, Hennessey WJ. "Sensitivity and specificity of carpal tunnel syndrome signs." Am J Phys Med Rehabil 1997 November; 76(6): 451-457.
Burke DT, Burke MA, Bell R, Stewart GW, Mehdi RS, Kim HJ. "Subjective swelling: a new sign for carpal tunnel syndrome." Am J Phys Med Rehabil 1999 November; 78(6): 504-508.
De SL, Steenwerckx A, Van den BG, Cnudde P, Fabry G. "Value of clinical provocative tests in carpal tunnel syndrome." Acta Orthop Belg 1995; 61(3): 177-182.
Neumann, Donald. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 2nd edition. St. Louis, MO: Mosby Elsevier, 2010. 219. Print.
Copyright © The Student Physical Therapist LLC 2023