
 Q&A with University of Southern California's Sports Residency Director: Dr. Aimee Diaz. Part 1: What makes your program unique? Part 2: What qualities do you look for in applicants? Part 3: What does a typical work week for residents include? Part 4: What type of jobs have resident graduates obtained? Part 5: Describe the faculty/mentors in the residency For more information on USC's Sports Physical Therapy Residency: http://pt.usc.edu/residency/sports/
2 Comments
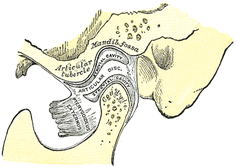 Recently, I had the pleasure of hearing Dr. Cohen, D.D.S. speak on the TMJ. Dr. Cohen is an Orofacial Pain Specialist that works out of the Phoenix area. As you may have noticed, we have not exactly covered the TMJ significantly before on this website due to what we thought was a low prevalence. However, as you'll soon see, it couldn't be further from the truth. For example, did you know that the American Dental Association does not require Dental schools to teach the temporomandibular joint? In fact, treatment techniques for TMJ issues by dentists (distraction, surgery to alter the bone/joint structure, etc.) often actually causes a greater TMJ issue or sometimes a TMJ issue that otherwise did not previously exist. As physical therapists, we are in an excellent position to screen for dysfunction at this joint and direct the patient to proper clinicians if appropriate. Anatomy and Kinesiology: The Temporomandibular Joint is made up of a posterior concave mandibular fossa and anterior convex articular eminence of the temporal bone that is combined with the convex condyle of the mandible. These surfaces are separated by an articular disc that is made primarily of fibrocartilage (this is important because this disc exhibits incredible self-healing abilities!). The disc reciprocally fits the TMJ in that the superior side is convex to match the concavity of the mandibular fossa and the inferior side is concave to match the mandibular condyle convexity (Neumann, 2010). The blood supply and innervation of the articular disc is somewhat debatable in that some say the entire disc is aneural (incapable of signaling pain), while others say only the middle third is aneural, leaving the anterior and posterior thirds with some innervation. With the joint being synovial, there obviously is a fibrous capsule that surrounds it as well. There are also several key ligaments involved with the joint, but that goes beyond the purpose of this review. There are two basic components of jaw opening and closing: rotation and translation. Basically, the first half of the motion occurs as a result of joint mechanics in the inferior side of the articular disc - the convex condyle rolls posteriorly and slides anteriorly (convex-concave rules!). During the second half, the superior part of the disc slides anteriorly on the articular eminence (Neumann, 2010). In general, the primary muscles of mastication include the temporalis, medial pterygoid, lateral pterygoid, and masster. The masseter is responsible for elevation of the mandible, slight protrusion, and, if unilateral, slight ipsilateral excursion. The temporalis elevates, retrudes, and, if unilateral, pulls the mandible ipsilaterally. The medial pterygoid is responsible for elevation and protrusion, while the lateral pterygoid is the only primary muscle that depresses the mandible (along with protrusion). Both muscles contralaterally deviate the jaw if acting unilaterally. It is worth noting that the superior head of the lateral pterygoid has fibers that attach to the capsule, suggesting an involvement with eccentric control of disc translation; however, the evidence is lacking on this. In addition, there are more than a few other muscles that are involved with TMJ function, the suprahyoid and infrahyoid muscles, but the reader is directed to other resources for further information in this area. 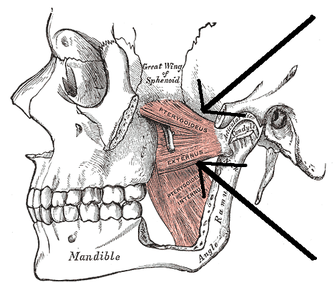
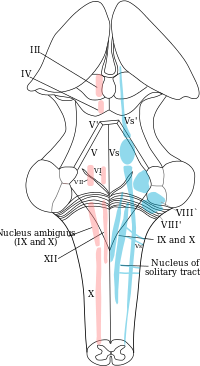
Signs and Symptoms: Some common symptoms of TMD include jaw/ear pain, headaches, ear stuffiness, dizziness, tinnitus, hearing loss, and jaw clicking. True TMJ pain can be identified by asking if the patient has pain with chewing. Remember, the disc is aneural, so the pain is not coming from the disc, but potentially the capsule, ligaments, or muscles involved. How can the ear be involved? The TMJ is connected to the ear's eustachian tube by the "Pinto's ligament." Any abnormal mechanics or pathology in the TMJ can stress the ligament causing ear pain, stuffiness, or even loss of hearing. Another potential cause for ear symptoms is the trigeminocervical nucleus and auriculotemporal nerve. (Fun Fact: Amoxicillin is often used for screening for ear infections. The problem with this is that Amoxicillin also contains an analgesic component. Antibiotics typically take 2-3 days to have effect. If a patient's ear pain subsides a couple hours after taking Amoxicillin, it's possible the TMJ was responsible for the ear pain). Headaches are often associated with TMD patients as a result of hypermobility in either the upper cervical spine or TMJ. Due to the lack of stability, the larger muscles are overused trying to hold the head up, thus causing a headache. This muscle tightness may instead exert excessive pressure over the trigeminal nerve or greater occipital nerve. When dizziness is involved, suboccipital tightness may result in compression of the greater occipital nerve or vertebrobasilar blood flow. Jaw clicking is a result of disc displacement in the TMJ typically. A history of jaw clicking can lead to the patient experiencing either an open or closed locked jaw. The closed locked jaw is related to an anteriorly displaced disc that does not reduce or a muscle spasm. Do not try and stretch these individuals open as you are likely to displace the disc even further forward. An open locked jaw is a result of a posteriorly displaced disc. The symptoms listed above are some of the more common symptoms related to Temporomandibular Dysfunction. Another important finding to consider is that of trigger points. Dr. Cohen spent extensive time discussing the relation of trigger points to headaches, TMD, and head/neck pain in general. If you have ever reviewed some of the trigger point referral patterns by Travell and Simons, you might realize that quite a few muscles have referral patterns to the head and neck that may mimic or contribute to TMD, headaches, etc. In fact, muscles like the temporalis can even refer to teeth, simulating a toothache (dentists may proceed to inappropriately pull a tooth out as a result). Trigger point injections often alleviate these symptoms immediately. While this is useful, remember this just treats the symptoms. We must treat the cause (often abnormal posture and the associated impairments). So be sure to assess trigger point contributions in your examination. Some treatment techniques by physical therapists may also be useful for this i.e. trigger point release, dry needling. Examination: When you are assessing an individual referred for TMD and cervicalgia, your examination should include both (along with the rest of the upper quarter). Some obvious thing to include are ROM, resisted isometrics, segmental mobility, palpation, listening for joint sounds (disc displacement), cotton roll test, and posture. ROM of the TMJ can reveal potential limitations of the capsule. Normal ROM is: 45 mm for depression, lateral excursion is 1/4 of depression, protrusion is 6-9 mm and retrusion is 3 mm (Ho, 2011). Lateral deviation to one side may signify capsular restrictions ipsilaterally, potential muscle dysfunction, or an anteriorly displaced disc without reduction ipsilaterally. This may be represented as a "C-curve" when opening (an "S-curve" is associated with hypermobility). Resisted isometrics can help you to identify a particular muscle that is not functioning properly. Segmental mobility of both the TMJ and upper cervical spine can potentially assist in identifying hyper- or hypomobility in a segment related to the abnormal mechanics. Palpation can be useful for assessing trigger points or tenderness in a capsule. The cotton roll test can help differentiate between muscular and joint involvement. If a patient complains of pain when chewing on one side of the mouth, have the patient bite down on a cotton roll. By doing so, this gaps the ipsilateral TMJ. Thus, if pain is decreased, it would appear the pain is joint related, but if it doesn't change or increases, the pain is muscular (it is still possible that the pain is related to the cervical spine as well). And of course, it all comes back to posture. Knowing the resting position of the teeth is important to understand the individual's TMJ mechanics and we have already discussed the impact cervical posture can have on the TMJ. Also, be sure to check for any poor habits such as bruxism, chewing on ice, grinding teeth, etc. that impact the TMJ.  Treatment: Treatment of TMD contains many of the methods that are regularly used for other joints and vary based on the impairments found and underlying condition. We must educate the patient on the pathology, postural correction, relaxation training for hyperactive muscles, and adjusting the patient's oral habits. Aerobic exercise can be useful in allowing relaxation of TMJ musculature and managing stress (Ho, 2011). The resting position of the mouth includes having the tongue on the palate of the mouth with the mouth closed and teeth not touching in a relaxed manner. Additionally, patients should be reminded to not bite nails, chew on pens, or continue other habits that affect the TMJ. In more acute cases, the patient should consume a softer diet and transition from chewing on the unaffected side to the affected side. Modalities may be used as indicated and joint/soft tissue mobilization can be used based on findings. As discussed before, trigger points can be treated with trigger point injections, dry needling, manual release, botox, etc. The home exercise program should involve retraining the patient on proper opening of the mouth. This is done by keeping the tongue on the roof of the mouth and slowly opening the mouth. This is useful because it prevents the anterior translation phase, thus preventing additional damage to the disc. The technique should be done regularly throughout the day. Isometrics to TMJ muscles are important for improving control of the joint, enhancing stability. Something that needs to be considered in TMD cases is splint therapy. The purposes include relaxing hyperactive muscles, reducing bruxing, altering clenching behavior, redistributing occlusal forces, preventing wear of enamel, and repositioning of a condyle (Ho, 2011). These splints are worn anywhere from constantly to just at night and may last up to 3 months or more. Due to the malleable effects splints have on the mouth, they need to be regularly adjusted. This brings up the important point of how modifiable the TMJ is. Dr. Cohen states that surgery and joint manipulation are the last options. The TMJ has the ability to adapt to changes and maintain full function for affected ligaments and muscles and sometimes even in cases like fractures. As stated several times before, we must include treatment of the cervical spine and entire upper quarter. Remember regional interdependence! This typically includes mobilization, manipulation, METs, etc. to restricted joints and cervical stabilization training. Anterior cervical muscles like the longus colli and longus capitis are often insufficient in patients with abnormal posture and require retraining. This strengthening/stretching/motor control training approach to postural muscles needs to be used down to the lumbar spine even, because poor core stability often leads to forward head displacement. This description of treatment techniques is a brief overview of how to manage patients with TMD. It is in no way all-inclusive. Each specific pathology may have a specific technique or exercise plan that has been shown to be especially beneficial. For example, there are specific exercise plans for displaced discs that are designed to retrain the muscles and recapture the disc in order to produce increased stability and motor control. The reader is advised to seek out other sources or the references for further information on these pathologies. Additionally, the outcome of patients with TMD can be improved with proper coordination with other health care practitioners like Orofacial Pain Specialists. The earlier these patients begin the conservative route, the more likely they will be able to avoid surgery. -Chris References:
Cohen, Richard. "Temporomandibular Dysfunction." Scottsdale Healthcare Orthopedic Residency Lecture. Scottsdale Healthcare Osborn Campus, Scottsdale, AZ. 21 Jan 2014. Lecture. Ho S. The Temporomandibular Joint: Physical Therapy Patient Management Utilizing Current Evidence. Current Concepts of Orthopaedic Physical Therapy, 3rd Ed. La Crosse, WI. 2011. Neumann, Donald. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 2nd edition. St. Louis, MO: Mosby Elsevier, 2010. 427-438. Print. Young PA, Young PH, Tolbert DL. Clinical Neuroscience. 2nd edition. Philadelphia PA: Lippincott Williams & Witkins, 2008. 145-149. Print. |
 RSS Feed
RSS Feed