
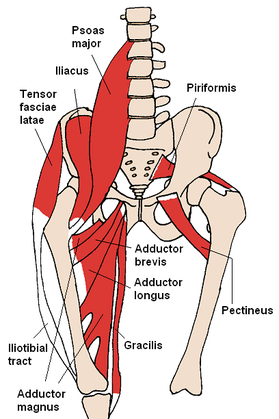
The iliopsoas is commonly regarded as a hip flexor, but it has two additional major functions: spinal compression and hip lateral rotation. The path of the muscle from origin to insertion begins on the lateral sides of the lumbar vertebral bodies, passes posterior to the vertebral column and then wraps posteriorly around the femur to the lesser trochanter. Acting as a spinal compressor, this muscle can be responsible for low back pain if short or stiff. Its role in lateral rotation can have a large impact on gait and jump mechanics as well. An individual that displays valgus knee positioning with squats often has weak hip abductors and lateral rotators. With the muscle wrapping around the femur posteriorly and acting as a lateral rotator, the iliopsoas is a muscle we definitely should consider in our intervention planning. This discussion lead me to realize the necessity of a 3-Dimensional understanding of our anatomy to further my knowledge in orthopaedics.
An example of anatomy's impact hit me with a patient in week 1. This patient presented with pretty clear signs/symptoms of a herniated disc. This patient described excruciating pain in her low back and hips after "trying to stretch her back and hamstrings out (this patient indicated she was doing so in a long-sitting method using primarily lumbar flexion)." She stated her pain is worsened by sitting and improved by standing/walking around. Pain increased and peripheralized with repeated lumbar flexion and centralized with extension. (+) SLR, Crossed SLR, and Slump Test. Following the evaluation, I prescribed prone press-ups, some core stabilization training exercises, and modification of lifting techniques. Stretching was deferred at this time as the patient was too acute and sensitive. At the follow-up visit a week later, the pain was mainly localized to the central spinal column, however her pain had switched from her posterior RLE to her L lateral thigh and inguinal area. This was somewhat an abnormal presentation to me, so I consulted my mentor. It turns out her distribution of her new symptoms were along the lateral cutaneous nerve at the lateral thigh, but also along the path of the nerve as it passes just inferior to the ASIS. The reason for the irritation lies in its lumbar innervation. This just happened to be an odd presentation as the pain switched extremities. So as you can see, it's not good enough to simply know what areas peripheral nerves and dermatomes contribute to and where the origins/insertions of muscles lie, but we must also strive to understand the path of the structures throughout the body. This will lead to improved clinical reasoning in both our examinations and interventions. -Chris
1 Comment
 How many of you are thinking about applying already to residency programs? If you are or think you may be in the near future, we recommend that you sign up for one of the webinars on August 6th or 7th to learn about the NEW centralized application system. Most of the residencies are participating in this process so it might be a good idea to get some details before you start applying!
See here for how to sign up. |
 RSS Feed
RSS Feed