
|
|
|
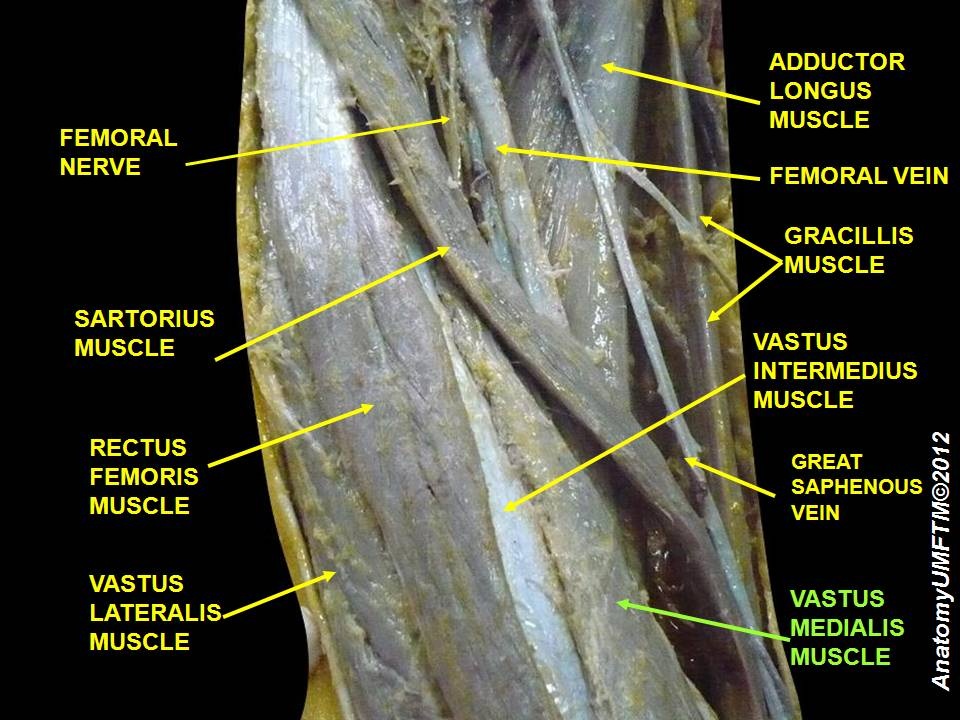
In regards to the nerve supply, the "nerves" often proclaimed as supplying the VMO or VML have been shown to be partitions of the femoral nerve to supply distal motor units, sensory nerves of the saphenous nerve, or nerve supply for the knee capsule. Additionally, let's take a look at the claimed function of the VMO: medial patellar tracking. No one has ever been able to demonstrate isolated medial patellar tracking. Many of the studies cited in this article are outdated. We are not disagreeing with the fact that different parts of the muscle have different proportions of fiber types, but we cannot come to the same conclusion of the significance of these findings. What are your thoughts on this recent article?
1 Comment
This is a good, quick 7-minute TED Talk given by the orthopaedic surgeon, Dr. Kevin Stone. He presents several interesting concepts and innovative strategies about the future of joint replacements. This might not be something you see in your clinical practice today, but as science continues to improve Dr. Stone's biological approach to joint replacements could be something you see on a more regular basis. Check it out!  We are all aware of the standard MMT for the gluteus medius in sidelying, but how well does this assessment transition to functional activities like walking? A sign we occasionally see is the Trendelenburg sign. This may consist of the uncompensated type (contralateral pelvic drop) or compensated type (ipsilateral trunk lean). Why not use Trendelenberg as a test as well? The Gait Guys had a recent post where they review this functional method of assessing gluteus medius strength. They include the various compensation methods to watch out for along with potential causes for the impairment. Check it out!
 As physical therapy students, much emphasis is placed on screening for Red Flags to help determine if a patient is appropriate for our services. Generally speaking, a Red Flag can be defined as a sign or symptom indicating the presence of a serious pathology. In a 2011 article, Davenport and Sebelski defined Red Flags as "abnormalities within the systems review...which may suggest the need for referral to another healthcare practitioner (Davenport 2011)." In this same article, these authors are quick to point out that Red Flags have a low predictive value for forms of pathology. A list of Red Flags commonly seen in the clinic are as follows:
With the profession of physical therapy on the brink of direct access and autonomous care, our ability to correctly determine a patient's appropriateness for therapy is crucial. A recent post from the ForwardThinkingPT outlines a 2013 Cochrane Review regarding the effectiveness of using red flags to screen for malignancy in the low-back pain population. The review assessed 8 cohort studies that specifically addressed 11 Red Flags in the patient's subjective interviews and physical examinations.* Of these 8 studies, which looked at >6000 patients, the symptom of low back pain presented as a more serious pathology <1% of the time. The review found that Red Flags associated with low back pain have high false positive ratings and that the "indication of spinal malignancy should not be based on the results of one single red flag question (Henschke 2013)." Despite the overall low probability of Red Flags, a few studies did find a meaningful increase in probability if the patient had a previous history of cancer. So where does this leave us as practitioners? It is important to consider that the Cochrane review only assessed the impact of 1 Red Flag in its relationship to increasing the chance of malignancy. In the clinic it is important to document Red Flags and use proper judgement if several of them are positive. Because of the high false positive occurrence, Davenport and Sebelski recommend utilizing a diagnostic process to help guide your clinical reasoning. This diagnostic process involves using a symptom based approach for diagnosis. With each patient you should ask yourself, "Among all possible health conditions, what is causing my patient's symptoms (Davenport 2011)?" Obviously this is a loaded question, but the question does stress the importance of having strong differential diagnosis skills. In conclusion, assessing for Red Flags can be a difficult process. Always remember to utilize good communication and practice forward-inductive reasoning to recognize patterns during your examinations. *It should be noted that all 11 Red Flag questions were not indicated in every chart and a possible limitation to the study is inadequate therapist documentation. References:
Davenport & Sebelski. (2011). The Physical Therapist as a Diagnostician: How do we, Should we, and Could we use Information about Pathology in our Practice? Physical Therapy. 2011;91.11. Web. 3 April 2013. Henschke N, Maher CG, Ostelo RWJG, de Vet HCW, Macaskill P, Irwig L. Red flags to screen for malig- nancy in patients with low-back pain. Cochrane Database of Systematic Reviews 2013, Issue 2. Art. No.: CD008686. DOI: 10.1002/14651858.CD008686.pub2. Web. 3 April 2013.
There are various types of stretching techniques: sustained, ballistic, proprioceptive neuromuscular facilitation (PNF), etc. They have the common goal of increasing musculotendinous length. Before considering which type is best, we must consider the properties of muscle. Muscles are composed of viscoelastic characteristics that can be influenced by stretch. The elastic component refers to the fact that a muscle has built in memory of it's original length. Just like the elastic part of your socks, given a temporary stretch, a muscle (or sock) will contract back into its resting length. That being said, with proper technique, a more permanent (or plastic) change in muscle length can be achieved. One of these techniques is a sustained stretch. But how long do we hold this stretch? In a classic study by Bandy & Irion, the researchers examined the difference in muscle length over time period of 6 weeks following sustained stretching programs based on time periods of 15, 30, and 60 seconds. A control group of no stretching was also followed. The study had several interesting findings. No significant differences in muscle length were found between the no stretching group and 15 second stretch group. This begs the question, what is the point of wasting time on a 15 second stretch, if there are no lasting effects. The results also found that significant gains were achieved with both the 30 second and 60 second groups, but minimal increase was found for the 60 second group. This means there isn't really a point of holding a stretch for 60 seconds either. The impact of this study displays the importance of reinforcing 30 second holds for stretches during a HEP. We often see our patients say they are holding a stretch for 30 seconds when in reality they are counting to 30 practically in one breath. It's no wonder they aren't seeing changes! 
As we mentioned before, there are several different methods of stretching with the most common being ballistic, sustained, and PNF. Ballistic stretching is not usually performed or recommended by health care practitioners due to its link to injury. The theory of ballistic stretching is to exceed the normal constraints of the muscle in order to achieve length increases, which suggests damaging the muscle. In regards to deciding between PNF and sustained stretch, there is still ongoing debate as to which obtains better results. O'Hora et al performed a study that looked at the immediate effects of 1 bout of PNF versus sustained stretch versus no stretch. The PNF stretch was a contract-relax maneuver of the hamstrings for 6 seconds. They found both PNF and sustained stretch to have significant changes in length following 1 bout. PNF changes were found to be greater than sustained. In the discussion, the authors reviewed the discrepancy in the literature regarding differences between PNF and sustained stretches, reminding the readers that there are many studies that have found each to be more effective than the other. An obvious issue with this study was the fact that the authors only looked at immediate effects of stretch and did not examine long-term effects. What can be taken from these findings and the discussion is that both 30-second sustained stretch and contract-relax can result in increases in muscle length. The debate goes on in regards to which is more successful. A combination we like to use is 3 sessions of contract-relax at end range, followed by a 30 second sustained stretch. References:
Bandy & Irion. (1994). The Effect of Time on Static Stretch on the Flexibility of the Hamstring Muscles. Phys Ther. 1994 Sep;74(9):845-50. Web. 6 April 2013. O'Hora J, Cartwright A, Wade CD, Hough AD, Shum GL. (2011). Efficacy of Static Stretching and Peripheral Neuromuscular Facilitation Stretch on Hamstrings Length after a Single Session. J Strength Cond Res. 2011 Jun;25(6):1586-91. Web. 6 April 2013.  Many physical therapy students and physical therapists are interested in private practice. While private practice can instill some independence with providing high-quality patient care, often physical therapists are still restricted in how we manage our patients. A solution to this problem is cash-based therapy. More and more frequently we are seeing clinics preferring to avoid insurance altogether or have an option of paying cash instead of charging insurance. With the current Medicare laws, patients who are Medicare eligible are not allowed to receive care in exchange for cash. Should a Medicare beneficiary run out of approved visits and want further treatment, they are out of luck. With the proposal of the Medicare Patient Empowerment Act of 2013, Medicare beneficiaries will be allowed to seek care privately from physical therapists and other health care professionals. Check out this APTA form to show your support for the bill!
 This is part 1 of Dr. E's blog post on treatment options to improve the overhead deep squat. Many components are involved in the deep squat which makes understanding the true cause of an inadequate performance difficult. The motion requires adequate hip extensor length, thoracic extension, ankle dorsiflexion, stability of the scapulothoracic musculature, and more. Both mobility and stability must be present in order to successfully complete the movement. With adaptive shortening of the hip extensors (especially the hamstrings), you often see difficulty maintaining proper lumbar position, leading to an excessively forward flexed torso. Thoracic extension and shoulder mobility combined with scapulothoracic stability are crucial for maintaining an upright posture while descending into the deep squat. Again, a deficit in this area often involves a forward flexed torso. Ankle dorsiflexion is necessary to prevent heel rise during the deep squat. We often see an adjustment for this in the FMS using the 2x6 wooden board to bring the ground up to the heels. Core stability is an obvious necessity as it contributes to maintaining proper posture during the movement. The components required for completion of the movement go on, but these are some common impairments.
Dr. E outlines 5 treatment options: 1. Thoracic spine manipulation to help improve thoracic mobility and glenohumeral motion. 2. Subscapularis Release for shoulder mobility. 3. Psoas Release: He demonstrates a great new video on a new psoas technique that is much less invasive and utilizes the principles of the neurophysiological effects of muscle tone. 4. IT Band Release using the edge tool to help increase hip mobility 5. Tibial Internal Rotation Mobilization with Movement for both knee and ankle mobility. He describes how the lower leg often is put into relative external rotation due to hip weakness, medial rotation of the femur, and pronation of the foot. He demonstrates each of these techniques with good clarity. Although he is using these techniques in relation to the overhead deep squat, you can see how they would apply to any patient with deficits in that region. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|

 RSS Feed
RSS Feed