
|
|
|
|
As physical therapists, we see many patients with a referring diagnosis of partial rotator cuff tear. Almost every patient with this pathoanatomic diagnosis will ask you one of these questions: "Can I injure it the tear worse? Will the muscle tear fully or recover? Will I need surgery?" These questions have complex answers with a myriad number of factors determining each answer. Below is a paragraph taken from the Orthopedic Physical Therapy Secrets book that should help answer the question, "Do partial rotator cuff tears heal or progress?" "1)Ruptured fibers can no longer sustain a load; thus increased loads are placed on neighboring fibers, making them more susceptible to rupture. 2) Disruption of the tendon fibers also disrupts local blood supply within the tendon, thus inducing ischemia. 3) Disrupted tendon fibers are exposed to joint fluid, which has a lytic effect on tendons that impairs the healing process. 4) When tendons heal, the scar tissue that replaces the ruptured tendon fibers does not have the same tensile strength as the original tissue; thus it is a increased risk of failure. 5) Once a tear becomes full thickness, loads that normally are distributed through the entire intact tendon often are transmitted at the torn margins of the rotator cuff tendon. This process produces a "zipper effect" and extends or unzips the tendon from the tuberosity. " From the information above, it is evident that in many instances, partial thickness rotator cuff tears progress to full thickness tears. The physiologic tissue structure following an injury has changed. The blood flow and tensile strength of that tissue has been permanently altered. It does appear that partial tears do progress. So where does this leave us? Fortunately, the physical therapy paradigm is shifting from a pathoanatomic to a pathokinesiologic model. Despite having a partial rotator cuff tear, patients can respond positively with conservative management. By addressing capsular mobility deficits, scapulohumeral strength and flexibility problems, and the presenting movement dysfunction, surgery is not always indicated following a rotator cuff tear. The Secrets book also states that variable amounts (33-90%) of individuals demonstrate improvements in pain and overall function despite having a full thickness rotator cuff tear. Not all patients will succeed with conservative management, but address your primary impairments and movement dysfunction and you will be able to decrease the patient's pain and improve their function. -Jim Heafner PT, DPT, OCS References: Placzek, Jeffrey D., and David A. Boyce. Orthopaedic Physical Therapy Secrets. St. Louis, MO: Mosby Elsevier, 2006. Print.
8 Comments
For various shoulder pathologies and movement impairment syndromes, one of the most common contributing factors includes a lack of sufficient scapular upward rotation. This is often due to insufficient activity of the trapezius and serratus anterior muscles. The serratus anterior muscle is capable of providing both a protraction and upward rotation force. It is the upward rotation force that we are wanting to test, however. In my clinical practice thus far, I have seen several different ways of testing the serratus anterior, but it is essential that the upward rotatory force is assessed. Origin: outer surfaces and superior borders of upper 8-9 ribs Insertion: costal surface of the medial border of the scapula Take a look at the video below for how to perform the MMT. How do you test the serratus anterior and what are some ways you like to train the muscle? -Chris Reference:
Kendall FP, McCreary EK, Provance PG, Rodgers MM & Romani WA. Muscles Testing and Function with Posture and Pain, 5th ed. Baltimore, MD: Lippincott Williams & Watkins. 2005. 332-333. Print.  Reading this title I'm sure you are wondering: What does your approach mean? I'll admit, its broad but what I want to cover in this post is how you interact with patients. Most importantly however, I want to talk about your subjective. Many of us have taken basic communication classes in PT school but they didn't help much. Practicing as a clinician for a 1.5 years and going through a residency as really made me re-think how I approach new and existing patients.
So what about the subjective exam? Well, for those of you that have studied pain science I'm confident you will agree that the way you go about interacting with the patient will make a big difference in that patient's outcome. Everyone has a different way they interact with patients and many times this can be influenced by the environment of the clinic you work in. However, you must still have your own unique approach. Think about that one PT you know that patient's love but really isn't doing any earth shattering treatment. Why do his or her patient's get better? Placebo? Possibly. We know that placebo's exist and have a certain effect on patients. Knowing this should make you think about how you interact with a patient. Eye contact, handshake, body position, and tone of voice all make a difference. How do you explain things to patients? Do you vary it depending on the level of understanding of the patient? How about the level of fear of the patient? Cueing is another thing. We could talk for hours on coaching cues but instead I'd rather have you watch this interaction with Gray Cook and Kelly Starett. They nail it. So now you're probably asking yourself, doesn't my patient's personality and/or approach make a difference? Glad you asked. It does. No matter what we think the patient needs, if that patient is not going to respond to that type of subjective or treatment, then it might be a waste of effort. Instead, learning what type of patient you have can make a big difference. Learn about their history, read their body language, and find out about past times in physical therapy. Now you can make a more meaningful impact. Ask yourself if you vary your approach depending on the patient. Then ask yourself how you interact with the patients your see and how you educate them. I really like this article by Zac Cupples for an in-depth approach on subjective interviewing. Worth checking out. - Brian Below is a great video that breaks down the fundamental components of the Ulnar Nerve. I will highlight a few key points, but I recommend watching the video as well. Ulnar Nerve Quick Facts: 1) The ulnar nerve originates from C8-T1 nerve roots. 2) It does not give off any branches in the axilla or upper arm 3) The nerve passes between the 2 heads of the flexor carpi ulnaris 4) Tinel's Sign can be used for assessing cubital tunnel syndrome 5) The nerve enters the palm through Guyon's Canal 6) The deep branch of the ulnar nerve innervates the three hypothenar muscles, two medial lumbricals, seven interossei, the adductor pollicis, and deep head of the FPB 7) The ulnar nerve provides sensory innervation to the little finger and half the ring finger 8) A claw hand deformity is due to unopposed pull of the flexor digitorum profundus. Enjoy the video!
-Jim 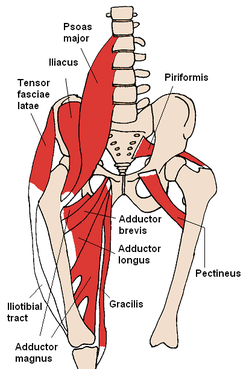 Last week, I evaluated a patient with neck and back pain s/p MVA. The patient presentation was pretty typical in regards to whiplash as far as aggravating and alleviating factors go. One thing that did stand out, however, was the presence of knee pain. The patient denied any trauma to the knee during the accident and has noticed it being far worse in sitting. This can lead one to a couple hypotheses, such as the presence of swelling with the knee in the 90 deg flexed position or neural tension causing the pain. Due to the lack of trauma and the patient not being able to pin point any one spot for the knee pain (medial knee pain into proximal medial tibia), I was leaning towards saphenous neural tension. As with any other hypothesis, additional testing is required to either increase or decrease likelihood. During my objective evaluation, I found several objective measures that increased my suspicion of a neural component at the knee: dysfunctional and painful lumbar extension and restricted lumbar sideglides to the involved side, positive slump test for reproduction of knee pain, no significant in findings of examination of the knee. Another finding that stood out to me was a reproduction of his knee pain with resisted hip flexion (not with palpation of the knee). This sort of finding brings to mind potential hip diagnoses such as SCFE, Legg-Calve-Perthes, Hip OA, etc., but the patient at arpproximately 40 years old didn't fall into the typical demographic for these pathologies. An additional explanation can be due to contraction of the Iliopsoas muscle. Remember the anatomy of the muscle: -Origin: (Psoas Major portion) ventral surfaces of the transverse processes of all lumbar vertebrae, sides of the bodies and corresponding intervertebral disks of the last thoracic and all lumbar vertebrae, and the membranous arches that extend over the sides of the bodies of the lumbar vertebrae; (Iliacus portion) superior 2/3 of the iliac fossa, internal lip of the iliac crest, iliolumbar and ventral sacroiliac ligaments, and ala of the sacrum. -Insertion: Lesser trochanter of the femur. The big thing to take away from the musculature attachments is the axial compression force that occurs with contraction. By compressing the spine, when the lumbar spine is irritated, neural symptoms can be produced, which is why the patient's pain was reproduced with neural tensioning. While the patient may benefit from some local treatment to the knee to decrease the neural symptoms, the primary focus of treatment must be on the back. Due to time constraints, I was unable to trial repeated motions, but that likely will be a significant part of my plan of care for both the neck and back pain, which may reduce the knee symptoms as well. -Chris References:
Kendall FP, McCreary EK, Provance PG, Rodgers MM & Romani WA. Muscles Testing and Function with Posture and Pain, 5th ed. Baltimore, MD: Lippincott Williams & Watkins. 2005. 422-423. Print. Patient’s primary complaint 48 y.o. male with Left elbow and upper extremity pain with upper extremity activity Physical Therapy Diagnosis Radial Nerve Tension with CT junction mobility deficits Subjective History General: On 10/1/14 the pt. presented to a PT clinic with L elbow pain during L elbow movements following a work related injury. He reports reaching to grab an object falling off a shelf weight approximately 10 lbs. Pain intensity was 4/10 and described as sharp and localized to the elbow. Work/Social: He has two jobs, primarily working at Lowe’s. Job duties include a range of tasks from prolonged desk work to lifting up to 30# in the different aisles. Other: Non-significant PMH, past surgical history. Denies taking any medications. From 10/1-10/6, he received two physical therapy treatments for the medical diagnosis of lateral epicondylitis. The original PT treated his lateral elbow pain with wrist stretching and strengthening exercises. The patient did not report any benefit and stopped attending PT. I first saw this patient on 12/2/14. He presented to my clinic with Left elbow pain and occasional referral from his common extensor mass to the lateral deltoid and down the arm to the dorsum of the wrist. Pain intensity was now 8/10 with arm and shoulder movements. He reported, “I thought I would give PT another try because my pain is so intense right now it is affecting my entire lifestyle- working, home activities…and sleeping.” Subjective history revealed his symptoms increase with elbow extension, wrist extension, pronation and shoulder flexion. His worst pain occurred with resisted elbow flexion and supination. Symptoms increase throughout the workday after using his arm. Additionally, he was now taking 200 mg Ibuprofen and Naproxen for pain management. This patient is L hand dominant. Objective Findings Postural Assessment: Forward head posture. Rounded shoulders with the L shoulder anteriorly displaced. Mini-CT junction hump with cervical hinging at C5-C6. Mild thoracic kyphosis. Left scapular protraction. Active Range of Motion: Cervical spine: WNL all movements, excessive hinging at C5-C6 with extension; Thoracic spine: decreased thoracic extension with no reversal of thoracic curve from T6-T8. Right UE: WNL. L UE: Shoulder Flexion, Abduction, Extension: WNL; Rotation (supine, arm abducted to 90 deg): ER: WNL, IR: grossly decreased. Elbow and Hand: WNL Passive Range of Motion: WNL all movements Joint Mobility: Hypomobility with right sideglides at C6-C7; Hypomobility and pain with PA assessment of T1-T3; Hypomobility with PA assessment from T6-T8. Hypomobility with posterior glides of GHJ; Hypomobility PA of the humero-radial joint. MMT: Deferred at initial evaluation (time constraints) Neurovascular screening: Vascular deferred (not applicable). Neuromuscular: Normal dermatomes and myotomes; +ive radial nerve tension test. Special Testing: +ive Cozen’s, +Mill’s Test, +ive resisted supination. Movement analysis (demo’ed with 5x shoulder flexion): cervical extension with shoulder flexion >120 degrees. Excessive scapular abduction during shoulder flexion, no reversal of thoracic kyphosis with shoulder flexion, decreased and poor coordination of L scapular retraction and downward rotation on return from flexion.
Asterisk Signs (12/2) Elbow flexion, supination AROM pain with movement: Pre-treatment: 8/10. Post-Thoracic and CT junction manipulation: 6/10. Post-C6-C7 mobilizations with radial nerve glides: 4/10. Post-treatment: 4/10. (12/5) Shoulder flexion pain with movement: Pre-treatment: 5/10. Post-treatment: 1/10 First Choice Intervention (with rationale) Manual Therapy: Supine Thoracic Manipulation- localized over T6-T8 -Neurophysiological Effects- reduction of neural tension, reflexive inhibition of periscapular muscles, hypoalgesic effects, decreased areas of activation in brain regions associated with pain (anterior cingulate, frontal cortex & sensory motor cortex) -Biomechanical: restore joint play and ROM within the thoracic spine, quick stretch of tight joint capsules -Psychological Effects- subjective report of relief with manipulation in the past. Second Choice Intervention (with rationale) Therapeutic Exercise: Radial Nerve Glides: -Improve axoplasmic flow within the nerve, improve nerve vascularization, improve the mechanical properties within the nervous system, facilitation of nerve gliding.
The patient has been on vacation for the past 3 weeks so I have not seen him since prior to Christmas. Assuming he is doing well, I am expecting 1-2 more treatment sessions for full return to work.
Conclusions: -We must perform appropriate differential diagnosis. The first PT improperly diagnosed his lateral elbow pain as lateral epicondylagia. The patient had months more duration of pain, increased medical cost, and time away from work. This could have been avoided with a proper differential. -Always assess the radial nerve in lateral elbow pain. -Look proximal and central when addressing nerve dysfunction. Many of this gentlemen's symptoms were due to poor posture and spinal mechanics. Hope you enjoyed the case. Send me any questions you may have. -Jim 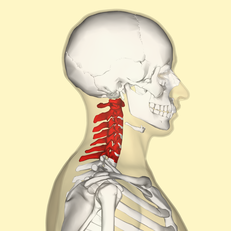 Jim and I recently had one of our Fellowship courses on the Advanced Cervical Spine. While practicing one of our cervical manipulation techniques, I realized I was having a protective spasm of some of my suboccipital muscles. This prevented Jim from getting my neck to end-range, which can be an important component of manipulations. I suggested trying a thoracic manipulation first to see if it would calm down the protective spasm. After the manipulation to T6, I had significantly less discomfort with the cervical positioning and Jim was easily able to get my neck to end-range. Jim was then able to complete a cervical manipulation with ease. There are multiple studies suggest thoracic manipulations can improve cervical dysfunction (Cleland et al, 2007) (Cleland et al, 2007) (Dunning et al, 2010). In fact, one of these includes a Clinical Prediction Rule that identifies patients with neck pain more likely to respond positively to thoracic manipulation. While thoracic manipulations are beneficial for neck pain, cervical manipulations can be even more effective (Puentedura et al, 2011) (Puentedura et al, 2012). While cervical manipulations have been shown to be more effective than thoracic manipulations for those with neck pain, they aren't always easy to perform. If the patient is experiencing acute neck pain, it's possible they cannot attain the position for manipulation in the cervical spine (as was the case for me). What these studies don't discuss quite as much is the benefit of using the two together. Like what happened to me, a thoracic manipulation can be used to possibly lower the pain threshold in order to do a more aggressive technique to the cervical spine. That being said, not every patient needs (or is safe enough for) cervical manipulations. You can also perform cervical mobilizations, MET's, or STM that would otherwise have been too uncomfortable. Some patient's will benefit from a thoracic manipulation alone. The point is treat the dysfunctions that you see as appropriate for your patient, but also consider using certain tricks that will permit you to have more direct approaches that the patient may be protecting again otherwise. -Chris References:
Cleland JA, Childs JD, Fritz JM, Whitman JM, & Eberhart SL. (2007). Development of a Clinical Prediction Rule for Guiding Treatment of a Subgroup of Patients with Neck Pain: Use of Thoracic Spine Manipulation, Exercise, and Patient Education. Physical Therapy. 2007 January;87(1):9-23. Cleland JA, Glynn P, , Whitman JM, Eberhart SL, MacDonald C, & Childs JD. (2007). Short-Term Effects of Thrust Versus Non-Thrust Mobilization/Manipulation Directed at the Thoracic Spine in Patients with Neck Pain: A Randomized Clinical Trial. Physical Therapy. 2007 April;87(4):431-440. Dunning JR, Cleland JA, Waldrop MA, Arnot C, Young I, Turner M, & Sigurdsson G. (2010). Upper Cervical and Upper Thoracic Thrust Manipulation vs Non-Thrust Mobilization in Patients with Mechanical Neck Pain: A Randomized Controlled Trial. Journal of Manual & Manipulative Therapy. 2010 December;18(4):175-180. Puentedura EJ, Cleland JA, Landers MR, Mintken P, Louw A, & Fernandez-de-las-penas C. (2012). Development of a Clinical Prediction Rule to Identify Patients with Neck Pain Likely to Benefit from Thrust Joint Manipulation to the Cervical Spine. JOSPT. 2012 July;42(7):577-592. Puentedura EJ, Landers MR, Cleland JA, Mintken P, Huijbregts P, & Fernandez-de-las-penas C. (2011). Thoracic Spine Thrust Manipulation Versus Cervical Spine Thrust Manipulation in Patients with Acute Neck Pain: A Randomized Clinical Trial. JOSPT. 2011 April;41(4).  I was recently performing an evaluation on a 27-year old male s/p car accident. He presented with classic whiplash signs and symptoms- neck pain, tenderness to palpation and hypomobility of the upper cervical spine, cervical joint restrictions, and high fear avoidance to movement. Additionally, he was having near constant headaches with reports of tinnitus and earaches. In this post I want to cover how and why ear symptoms can be related to both upper cervical and TMJ Dysfunction
Cervical nerves 1-3 and cranial nerves V, VII, IX, X, and XI all meet at the trigeminocervical nucleus. These nerves are in very close proximity to one another. When dysfunction occurs in one of the nerves, the other nerves can receive abnormal inputs as well. The TMJ is innervated by the mandibular division of the Trigeminal Nerve (cranial nerve V) and is therefore at risk. The mandibular division further branches into the deep temporal nerve, masseteric, and auriculotemporal nerves. Since the auriculotemporal nerve is responsible for innervating the tempanic membrance and the external auditory meatus, dysfunction of the TMJ can cause ear symptoms. On the same note, the upper cervical nerves exit around the suboccipital triangle, giving the possibility of a cervical patient to have ear symptoms. In my car accident patient described above, I have been focusing heavily on patient education, proper body mechanics, relaxation techniques, and upper cervical joint mobility. By improving upper cervical mobility, the upper cervical nerves can be taken off tension. Therefore the trigeminocervical nucleus will stop receiving poor inputs and indirectly stop affecting the auriculotemporal nerve. Within 3 visits, he continues to have headaches, but his ear symptoms have subsided! -Jim  Looking back at our content over the past year has been fun. All three of us have developed professionally. We have graduated from residency programs, Chris and I are pursuing fellowships in manual therapy, and we have launched our premium page! Our content is becoming more diverse and more advanced with each post. Here is a quick review at the top 5 posts (ranked by Facebook likes and comments) over the 2014 year. In no particular order
5) Exercise Protocols: Why They Work often Work and Why We Must be Careful In general, many patients fall into typical pattern with similar impairments. Knowing the common patterns may allow you to speed up the process, but if you ignore the exceptions, you will fail to make progress. Always Test, Treat, Re-test! 4) Are You Hamstring Dominant? As I have grown as a clinician, I have recognized the importance of motor control more and more. Testing for hamstring or lumbar dominance over the gluteals is very important. Do not be fooled by strong gluts in the low back pain population. After assessing the glut max, retest for hamstring dominance to ensure they are not over-activating the hamstrings. Dominance patterns are extremely common. 3) Plantar Fasciosis or Lateral Plantar Nerve Pain As our clinical skills have improved, so has our differential diagnosis. Assessing for nerve pain in the presence of common musculoskeletal conditions has become part of every one of my examinations. In all patients that present with plantar fasciosis, you must check the lateral plantar nerve as well! 2) ATFL Sprain or Neural Tension? No surprise here! Just as I stated you must assess the lateral plantar nerve in plantar fasciosis, it is equally important to assess the intermediate dorsal cutaneous nerve in lateral ankle sprains. Read this post to learn more about the IDC nerve and how to test for neural tension. 1) Repeated Motions Exam: Why you Should be Using It. Many of Chris' recent posts have included repeated motions. In school they are often overlooked and misunderstood. Clinically, they can be difficult to assess your accuracy because the position is pain provoking. Do not let these factors stop you from learning about and using repeated motions. Read this post to get you started! Thank you to all of our readers. We enjoy writing for you and learning from you with your comments and feedback. Jim Heafner |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|



 RSS Feed
RSS Feed