
|
|
|
"Hinge points and movement deviations may not be pertinent to pain, but they tell a story about how someone chooses to load their joints and program their movements." |
 |  | 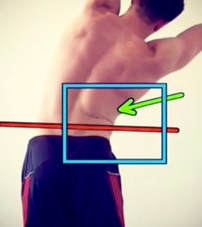 |
Picture Analysis
*Do not worry pain scientists, I know we naturally flex through the lumbar spine and some people naturally lean more forward depending on their tibia to femur ratio.
**Do not worry global strengthening folks, I know there is no evidence to support TrA activation.
***I won't get into the topic of inhibited vs. facilitated muscle groups in this post.
- Hinge point in R low back at L2 region with side bending
- Excessive lumbar flexion with forward trunk positioning during the squat
- Hinge point at L2 region during lat pull down
*Do not worry pain scientists, I know we naturally flex through the lumbar spine and some people naturally lean more forward depending on their tibia to femur ratio.
**Do not worry global strengthening folks, I know there is no evidence to support TrA activation.
***I won't get into the topic of inhibited vs. facilitated muscle groups in this post.
Pain Science Perspective
I am aware that hinge points and movement deviations on a squat are not a cause of pain. As I wrote in a blog post earlier this year, "The research does not support either good or bad posture. We cannot confidently say that poor posture causes problems OR good posture prevents problems. This is because posture alone does not equal pain. Several studies have been published over the past few years that confirm pain is unrelated to our anatomical tissues. For example, 34% of asymptomatic people >60 years old have been found to have rotator cuff tears. One in three people WITHOUT SHOULDER PAIN have a rotator cuff tear. "
However, I simply could not do enough self-neuroscience education to decrease the pain (maybe I didn't believe myself...who knows.) Despite offloading and gradually reintroducing weight to the movements, my brain continued to recognize the movements as painful.
However, I simply could not do enough self-neuroscience education to decrease the pain (maybe I didn't believe myself...who knows.) Despite offloading and gradually reintroducing weight to the movements, my brain continued to recognize the movements as painful.
At this point, I hit a crossroad. Do I...
1) Continually load the painful patterns to desensitize the movements
- This would follow the pain science path of treatment
- This would follow the movement and posture path of treatment
Self Treatment
Personally, I chose to perform a combination of both options.
My top 3 interventions:
My top 3 interventions:
- Lumbar extensions
- Hip external rotation mobility
- Thoracic mobility.
 |  |  |
1) Lumbar extensions were performed to improve lumbar extension range of motion as well as improve the loading pattern into extension as I squatted. While the first few repetitions were painful, the repeated loading desensitized movement and allowed me to maintain an upright position in the squat.
2) Hip External Rotation mobility was performed to improve the joint mobility in my hips. I perceived that tight hip joints were limiting my capacity to squat. From a mechanical standpoint, improved hip mobility allowed me to disassociate lumbar motion from pelvic motion. The increased hip mobility allowed me to maintain a neutral spine position and load through the posterior chain.
3) Thoracic mobility was performed to help maintain an upright posture during squatting movements and allow for improved shoulder mobility while performing lat pull downs. Additionally, improved thoracic mobility gave me a sense of better scapular muscle activation.
2) Hip External Rotation mobility was performed to improve the joint mobility in my hips. I perceived that tight hip joints were limiting my capacity to squat. From a mechanical standpoint, improved hip mobility allowed me to disassociate lumbar motion from pelvic motion. The increased hip mobility allowed me to maintain a neutral spine position and load through the posterior chain.
3) Thoracic mobility was performed to help maintain an upright posture during squatting movements and allow for improved shoulder mobility while performing lat pull downs. Additionally, improved thoracic mobility gave me a sense of better scapular muscle activation.
Incorporating Movement & Pain Science
In my situation, combining my knowledge of pain and tissue damage with the more mechanical approach of proper alignment was very effective. Since the brain is the control center of all input and output, it recognizes when someone is using too much energy to perform a task. For example, the forward head posture is not inherently painful, but chronic forward head positioning is an inefficient use of energy. To hold the head in a forward position, the anterior and posterior muscles are not working in equilibrium. The brain must expend more energy, time, and attention to keeping the head in a forward position. It has nothing to do with pain, and everything to do with efficiency. The combination of approaches was beneficial because I brought awareness and perception to areas that needed stimulation, and simultaneously calmed down areas that were already too sensitive to movement.
In conclusion: the treatment approach will be different for everyone. We all think, move, and act in unique ways. Many of our daily actions are performed reflexively without thought or awareness. Bringing increased perception to a painful region while modulating their pain will allow someone to understand why the pain is occurring and how to control symptoms.
In conclusion: the treatment approach will be different for everyone. We all think, move, and act in unique ways. Many of our daily actions are performed reflexively without thought or awareness. Bringing increased perception to a painful region while modulating their pain will allow someone to understand why the pain is occurring and how to control symptoms.
-Jim Heafner PT, DPT, OCS
1 Comment

Core strengthening appears to be a very abstract term in the world of physical therapy. To some, it means very specific motor control training. To others, it means planks. Several years ago, a proposed core stabilization clinical prediction rule was shown to lack validity. Regardless, due to the lack of established guidelines for core stability training, there will continue to be a variety of techniques, based on the clinician's preference.
When it comes to lumbar manipulation, there has been a significant amount of research to show our inability to manipulation a specific segment. Even when we try to "isolate" an area, movement can occur several segments above and below. It would appear the lack of specificity with manipulation is rather insignificant, so certain patients may just respond to manipulation in general. Can the same theory apply to stabilization? I recently read a study that compared specific motor control training in the lumbar spine to high-load deadlift training. The results showed that there was no difference in strength, pain intensity or muscle endurance between the two groups. The motor control group did have better motor control and activity, but the fact that pain, strength, and endurance were similar can help us in not needing to be so specific with our exercises. Sometimes, the particular instructions we give to our patients can actually cause a fear of movement, which is something we want to avoid.
When it comes to lumbar manipulation, there has been a significant amount of research to show our inability to manipulation a specific segment. Even when we try to "isolate" an area, movement can occur several segments above and below. It would appear the lack of specificity with manipulation is rather insignificant, so certain patients may just respond to manipulation in general. Can the same theory apply to stabilization? I recently read a study that compared specific motor control training in the lumbar spine to high-load deadlift training. The results showed that there was no difference in strength, pain intensity or muscle endurance between the two groups. The motor control group did have better motor control and activity, but the fact that pain, strength, and endurance were similar can help us in not needing to be so specific with our exercises. Sometimes, the particular instructions we give to our patients can actually cause a fear of movement, which is something we want to avoid.
Now, I am not necessarily saying there is no point to motor control training. I would simply argue that it's not as important as we used to think. If there is a subtle pelvic motion when reaching overhead, we don't necessarily need to be stopping the exercise altogether. It may still be beneficial to establish some general patterns of motion during earlier stages of rehab in order to prevent re-aggravation during high load training. Personally, following my manual treatment (if indicated), I will start with a couple mobility exercises to help get the spine moving. I then follow that up with some motor control training to prep for whatever movement I am going to have the patient perform. For example, if my patient will be doing a deadlift, I will prime them with a quad rock back and/or hip hinge, in order to help dissociate lumbar and hip motion with heavy lifting. My end-goal however, is to get my patient strengthening with heavier weight.
-Dr. Chris Fox, PT, DPT, OCS
-Dr. Chris Fox, PT, DPT, OCS
TSPT is now offering a comprehensive LUMBAR SPINE COURSE
Interested in learning more about the lumbar spine?
 | This online course includes:
|
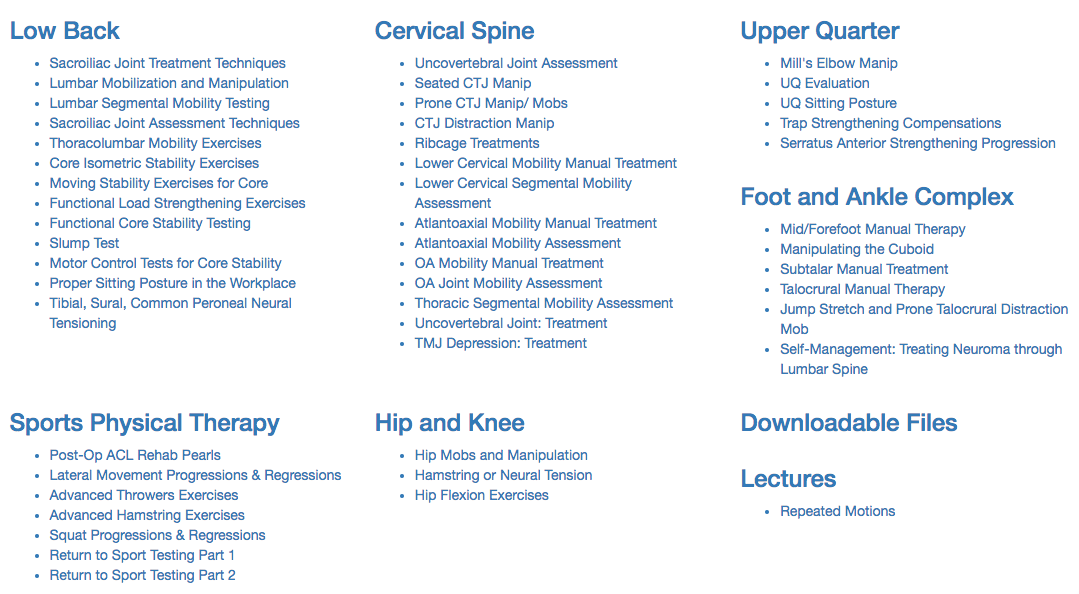
Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly.
Cervical stability testing is one of the most important aspects of a cervical screen. While it may not help our treatment directly, it may save some people's lives or prevent significant worsening of injury. There are several key components of cervical stability testing:
-Transverse Ligament
-Alar Ligament
-Fracture Screening
There is specific testing for Alar Ligament Integrity but for cervical fx screening, it is recommended to utilize the Canadian C-spine rules and Jefferson Fx test.
The Transverse Ligament is responsible for maintaining stability between C1 and the odontoid process of C2. Without the ligament functioning, spinal cord injury is possible. While it is rare for a patient with a ruptured Transverse Ligament to present to you in a clinic, with direct access, it is certainly possible. The patient may hold their head in a certain position (avoiding positions that aggravate symptoms), to keep the injury "reduced." There are two methods that we recommend for testing the ligament's integrity: Sharp-Purser Test and Supine Transverse Ligament Test.
-Transverse Ligament
-Alar Ligament
-Fracture Screening
There is specific testing for Alar Ligament Integrity but for cervical fx screening, it is recommended to utilize the Canadian C-spine rules and Jefferson Fx test.
The Transverse Ligament is responsible for maintaining stability between C1 and the odontoid process of C2. Without the ligament functioning, spinal cord injury is possible. While it is rare for a patient with a ruptured Transverse Ligament to present to you in a clinic, with direct access, it is certainly possible. The patient may hold their head in a certain position (avoiding positions that aggravate symptoms), to keep the injury "reduced." There are two methods that we recommend for testing the ligament's integrity: Sharp-Purser Test and Supine Transverse Ligament Test.
| | |
While both tests can be effective for assessing stability, we recommend using both. First, the Sharp-Purser Test should be used as it is a REDUCING test. That means, if a symptomatic patient presents, you will reduce their symptoms if the test is positive. While most patients won't allow you to "provoke" their symptoms with the initial part of the test, it is still important to try reducing symptoms before aggravating. Next, we recommend using the supine Transverse Ligament Test to provoke symptoms. The force is minimal, so it is unlikely to be harmful if stopped when any appropriate symptoms are produced.
While the diagnostic accuracy for upper cervical stability and utilization of Canadian C-Spine rules is relatively high, it is not recommended to completely override clinical decision making. As always, we recommend a thorough evaluation and consideration of the evidence of each test's findings. For more information on these tests, be sure to check out the pages linked above.
-Dr. Chris Fox, PT, DPT, OCS
While the diagnostic accuracy for upper cervical stability and utilization of Canadian C-Spine rules is relatively high, it is not recommended to completely override clinical decision making. As always, we recommend a thorough evaluation and consideration of the evidence of each test's findings. For more information on these tests, be sure to check out the pages linked above.
-Dr. Chris Fox, PT, DPT, OCS
TSPT now offering a comprehensive Cervical Spine Course
Interested in learning more about the cervical spine?
 (Save $10 with Promo: Neckpain) | This online course includes:
|
Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly.
In honor of National Physical Therapy month, The Student Physical Therapist has compiled a list of facts, statistics, and fun information about our amazing profession. This quiz covers everything from historical facts about Physical Therapy to Physical Therapists perception on the dating app Tender!
 |  |
 |  |
Take our Quiz!
We hope you enjoy the quiz! Please continue to strive everyday to make the profession great.
#getPT1st
Jim, Chris, and Brian
#getPT1st
Jim, Chris, and Brian
Join the Insider Access Community!
 | Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added regularly. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages
Insider Access pages


We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!
Archives
July 2019
June 2019
May 2019
March 2019
February 2019
January 2019
December 2018
November 2018
October 2018
September 2018
August 2018
July 2018
June 2018
May 2018
April 2018
March 2018
February 2018
January 2018
December 2017
November 2017
October 2017
September 2017
August 2017
July 2017
June 2017
May 2017
April 2017
March 2017
February 2017
January 2017
December 2016
November 2016
October 2016
September 2016
August 2016
July 2016
June 2016
May 2016
April 2016
March 2016
February 2016
January 2016
December 2015
November 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
February 2015
January 2015
December 2014
November 2014
October 2014
September 2014
August 2014
July 2014
June 2014
May 2014
April 2014
March 2014
February 2014
January 2014
December 2013
November 2013
October 2013
September 2013
August 2013
July 2013
June 2013
May 2013
April 2013
March 2013
February 2013
January 2013
December 2012
November 2012
October 2012
September 2012
August 2012
Categories
All
Chest
Core Muscle
Elbow
Foot
Foot And Ankle
Hip
Knee
Manual Therapy
Modalities
Motivation
Neck
Neural Tension
Other
Research
Research Article
Shoulder
Sij
Spine
Sports
Therapeutic Exercise
 RSS Feed
RSS Feed