
|
|
|
|
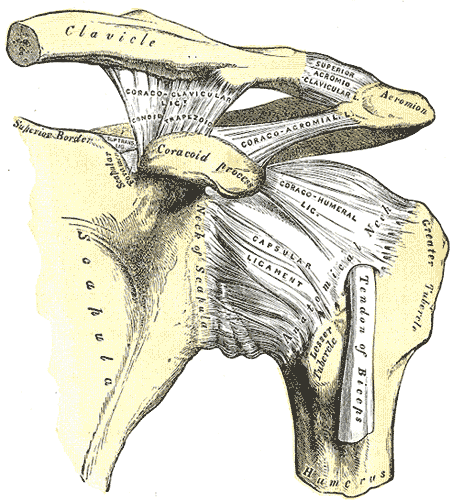
The shoulder is a complex region of the body as it is comprised of several different joints: glenohumeral, sternoclavicular (SC), acromioclavicular (AC), and scapulothoracic. In this post I will primarily be discussing the AC joint anatomy, joint mobility, and how to address movement restrictions in this region.
Kinematics The AC joint is primarily responsible for subtle adjustments of the scapula relative to the clavicle. The scapula upwardly rotates at the AC joint during shoulder flexion and abduction. It downwardly rotates during extension and adduction. With the horizontal plane, the AC joint permits some internal and external rotation. Additionally, the AC joint has slight anterior/posterior titling in the sagittal plane. It is important to remember that the majority of the AC joint kinematics are pretty minimal. Not much motion occurs here at all, but it is still important. Assessment and Treatment The AC joint is often responsible for the end-range elevation mobility in the shoulder. While this joint should always be assessed, it should definitely be considered when elevation mobility is restricted. Should there be an actual injury to the AC joint, it typically will present as pain over the joint and possible visual deformity. There are also several tests for AC joint injury, a couple (Active Compression Test and Horizontal Adduction Test) of which are shown below:
However, the AC joint is important to assess in non-AC joint shoulder pain as well. Consider the regional interdependence concept on a smaller scale: restriction in the AC joint or SC joint may lead to excessive motion and pain in the GH joint. Due to the planar alignment of the joint surfaces, it is recommended that a gliding assessment is used to simply determine if the area is moving or not. We will recommend using the directions of anterior-posterior and posterior-anterior when assessing to identify joint mobility stiffness. If restricted, you can use the same technique to mobilize it or some of the other ones shown in the video below: FREE PREVIEW OF THIS MONTH'S INSIDER ACCESS: AC JOINT MANUAL ASSESSMENT AND TREATMENT To help improve or retain mobility in the AC joint, I recommend some general mobility exercises or possibly some upper trap/serratus anterior strengthening to facilitate end-range elevation.
For more videos like this one on the AC joint, be sure to subscribe to Insider Access! -Dr. Chris Fox, PT, DPT, OCS
0 Comments
 It's that time of the year again when nerves start to settle in for those who are taking this July's NPTE exam. I remember very distinctly the days leading up to the exam and I am sure you all share some of the same feelings. Am I ready? Did I study enough? Can I withstand the long test? Don't worry, these feelings are all normal. Chances are, you are more than prepared. You finished physical therapy school (which isn't easy) and you completed clinical rotations. That in itself is great prep for your exam. On top of that you've been studying for at least the last few weeks (hopefully). You're not going to be able to memorize or remember everything and thats OKAY. Nobody can remember everything and there will be some questions that you going to say "WHAT?". But rest assured, some of those questions are going to be thrown out because they are test questions for future exams. Still not convinced you did enough? Let me tell you about my story. I got into USC's sports residency in May of 2013. However, because my school's graduation date was after the date to apply for an out of state exam (I had to get finger printed, etc for California) I was not allowed to take the July exam. Which meant I had to stop studying and wait until October. Then, in late June I got a call that I'd been approved for the July exam after multiple people called on my behalf. Which meant that I had less than a month to study for this exam, move to California, get an apartment, and then take the exam! My final days before the exam were spent flying to Los Angeles, picking up my car 45 minutes away that I had shipped with all my stuff, and studying in between my Dad and I putting my apartment together to be functional. So trust me, you will be fine! Final Tips for the last week: - Review what you feel least comfortable about - Go to bed at the same time and wake up at the same time to get your body used to exam times - Get some good workouts in but don't exhaust your body - Don't experiment with any new food or drinks - Find something to take your mind off of the exam the night before (ex: a movie) - Wake up exam day and commit your mind that no matter what is thrown at you, today you are going to find a way to get the answers correct Good luck to all that are taking the NPTE! Dr. Brian Schwabe, PT, DPT, SCS, COMT, CSCS   So much information...so little time!!!The final weeks before the July 2018 NPTE exam are upon us! While this post is not about how to study, I do want to include my TOP piece of advice: As a general rule, I cannot stress enough the importance of taking practice exams and analyzing each question (both incorrect and correct answers). I took five or more practice exams and looked through every question thoroughly. Multiple times I found myself answering questions correctly, but using the wrong clinical reasoning. Other times, I would answer a question incorrectly, but had the proper thought process. These reviews will solidify the information you know and significantly improve your weak points. To read more about how Chris, Brian, and I prepared for the exam, click HERE. Whether you have been studying for 3 months, 3 weeks, or 3 days, this post is a friendly reminder to spend a little extra time on 3 important subjects. I break down each one below! Topic #1: Sensitivity, Specificity, and Likelihood RatiosWhile the direct 'research based' questions are <5% of the examination, it is important to know the difference between sensitivity, specificity, and likelihood ratios. These metrics are commonly seen on various examination techniques, and give practitioners an idea regarding how beneficial that test is clinically. Sensitivity refers to a test's ability to accurately rule out a disease and is scored between 0 and 1.00. Tests with high Sensitivity, rule Out a disease (SnOut). Specificity refers to a test's ability to accurately rule in a disease and is scored between 0 and 1.00. Tests with high Specificity, rule In a disease (SpIn). Positive and negative likelihood ratios work in a similar way but are not limited to numbers between 0 and 1.00. They act more as "persuasive information" and are more individualized than sensitivity and specificity (Jewell, 2010). Clinicians are required to determine a patient's pretest probability, then incorporate the likelihood ratio for the test and determine how "likely" the patient has the pathology. Keep in mind that the diagnostic accuracy applies to a specific patient population, and will change as other variables change. For example, the sensitivity and specificity of the Lachman's test is largely different in the acute phase of injury versus the chronic phase. Below is an example question from PT Final Exam: If a magnetic resonance image (MRI) correctly identifies 95% of patients as positive for anterior cruciate ligament tears, then the MRI is:
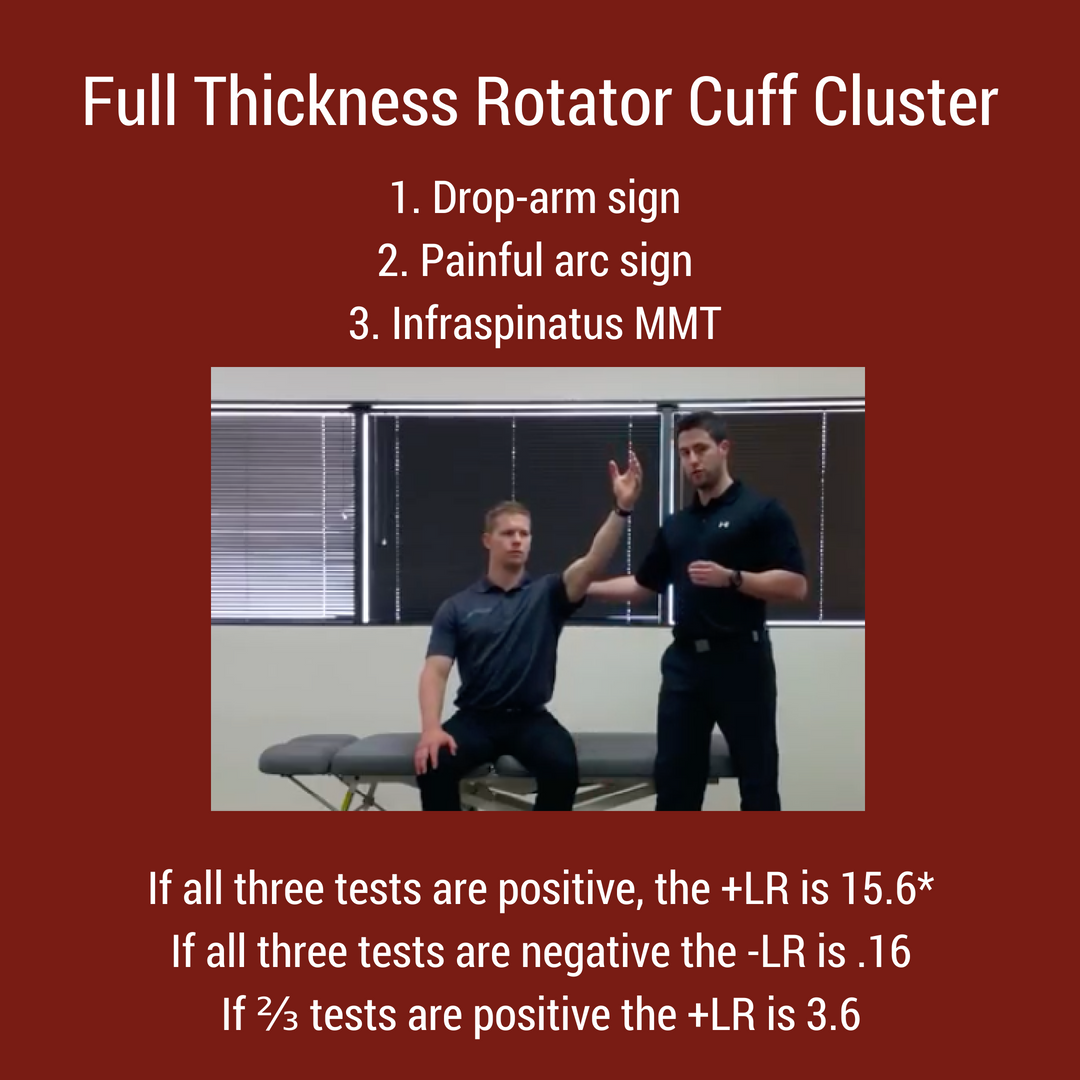
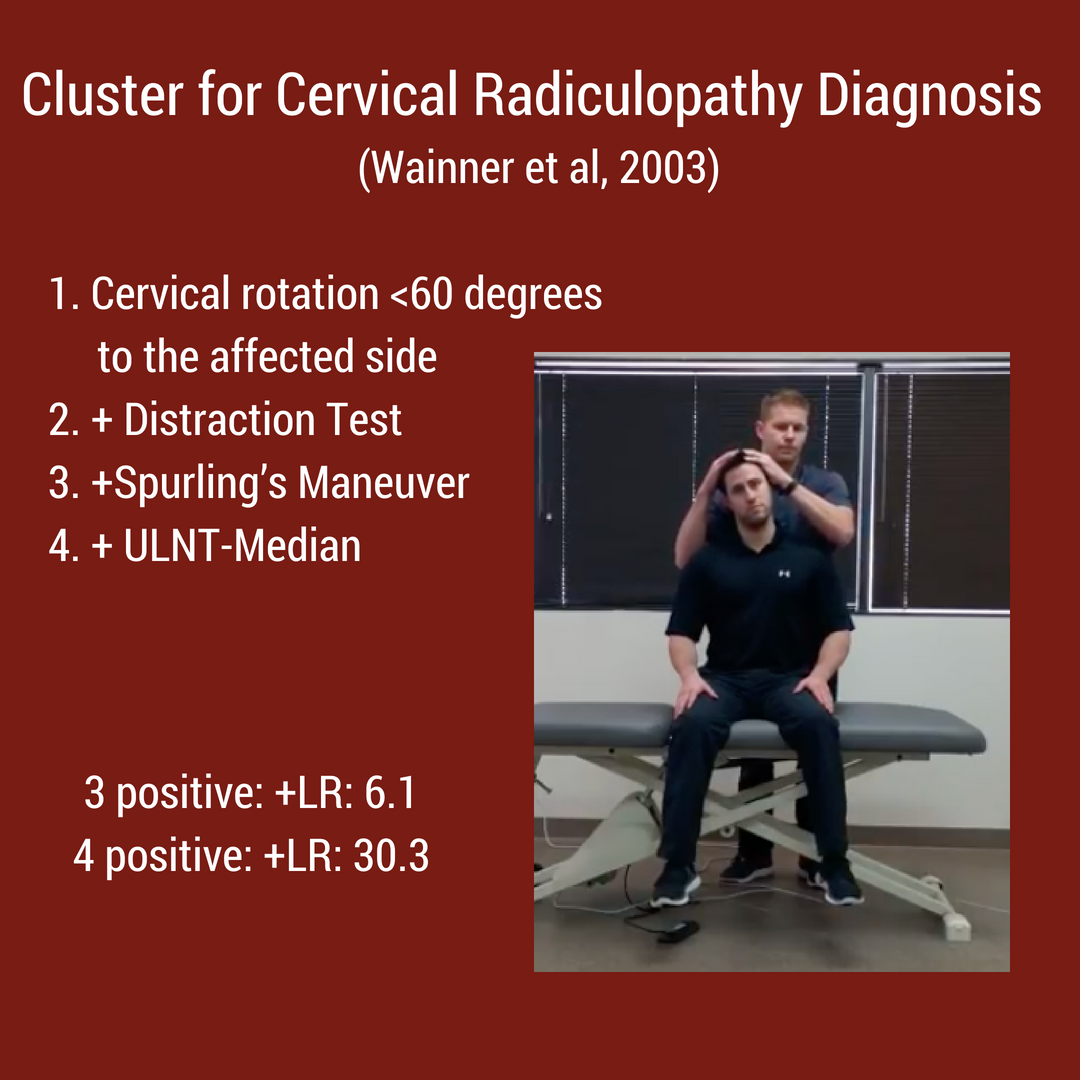
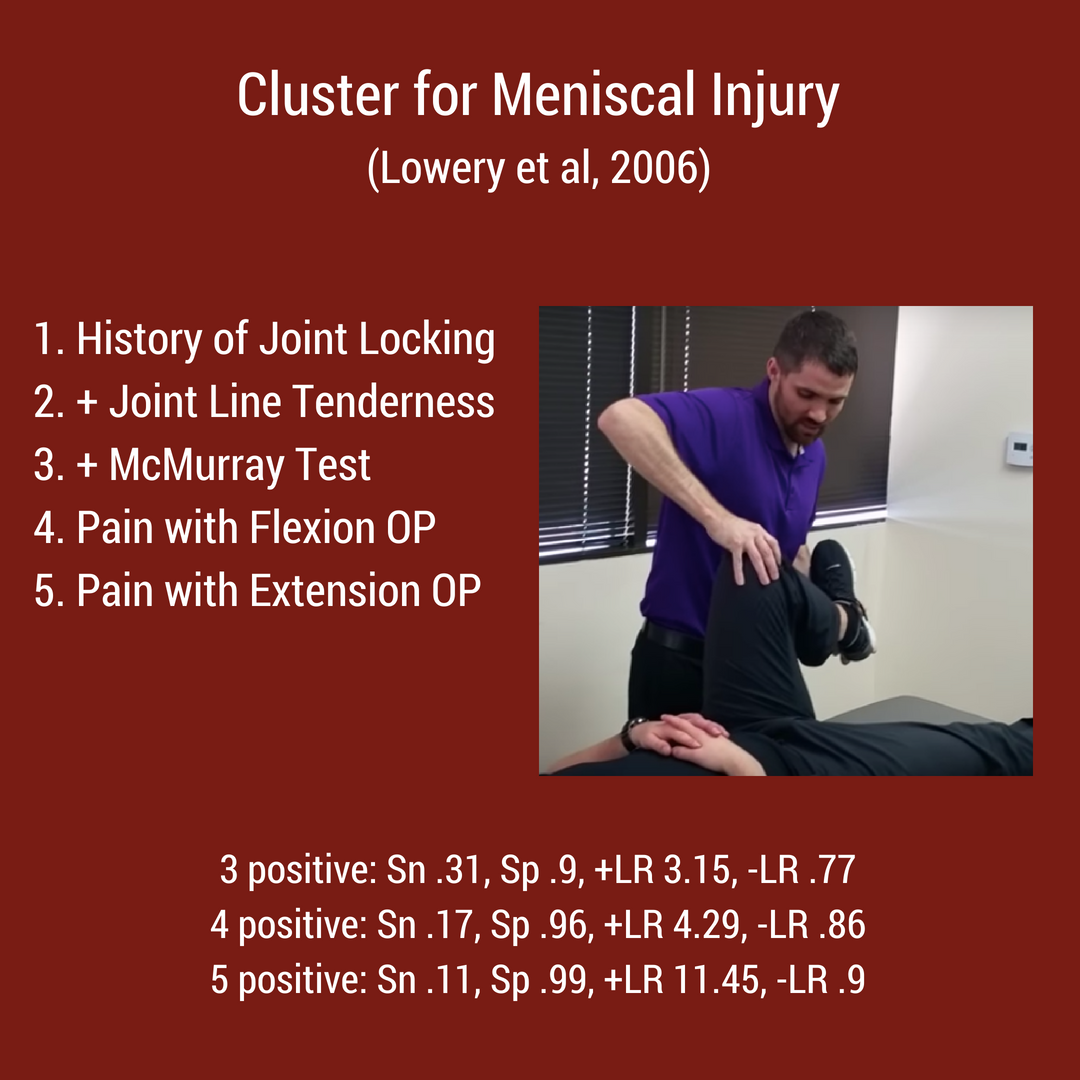
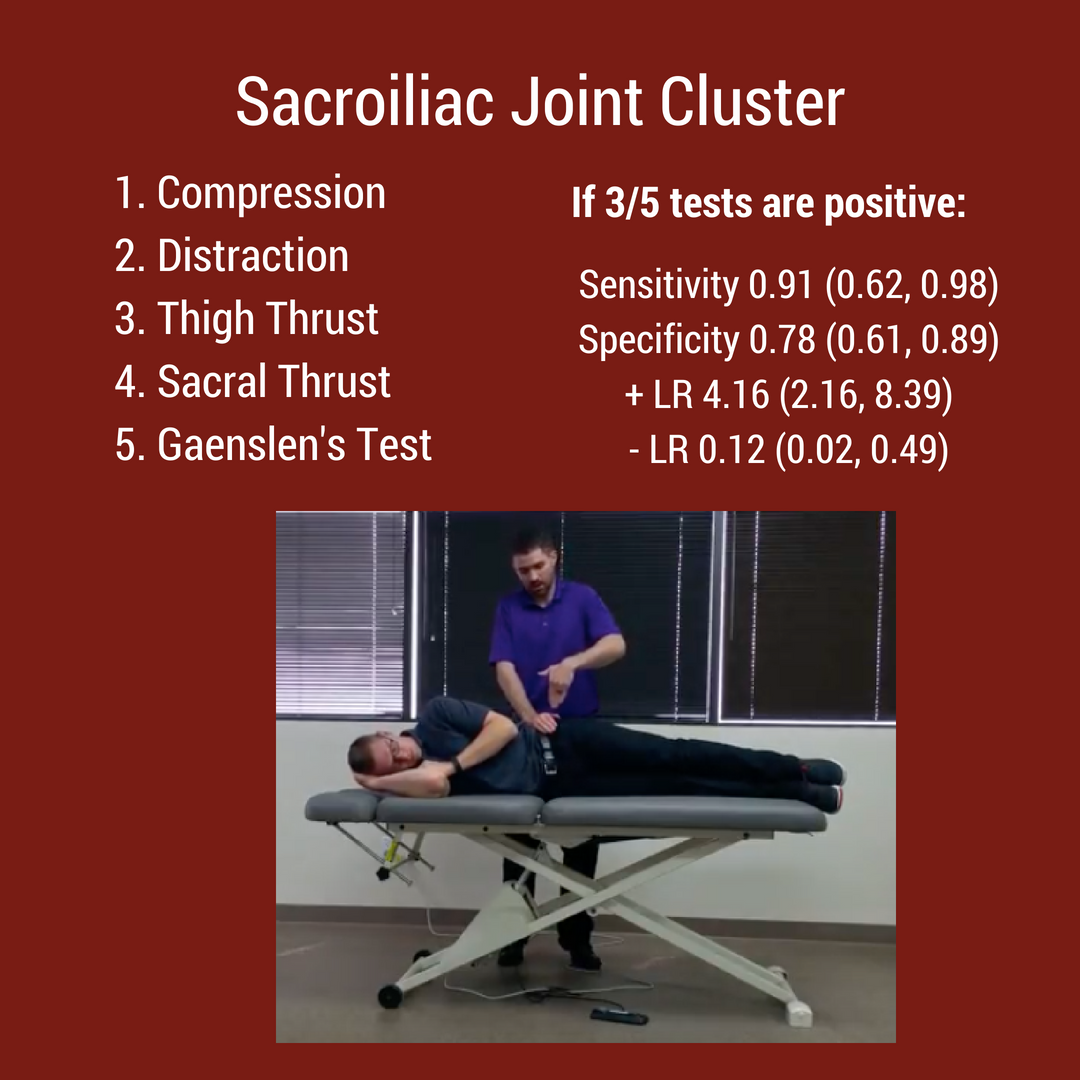
 Topic #2: Special Test ClustersFrom the rotator cuff to the menisci, there are multiple special test clusters that exam participants must review. While these tests may lack good diagnostic accuracy individually, when clustered together, their ability to diagnosis tissue pathology significantly improves. In addition to the special test clusters, I highly recommend looking at Wells Criteria for a Deep Vein Thrombosis, the Ottowa foot and ankle rules, and hip/ knee arthritis criteria. Below are 4 major clinical clusters that are important for the NPTE.
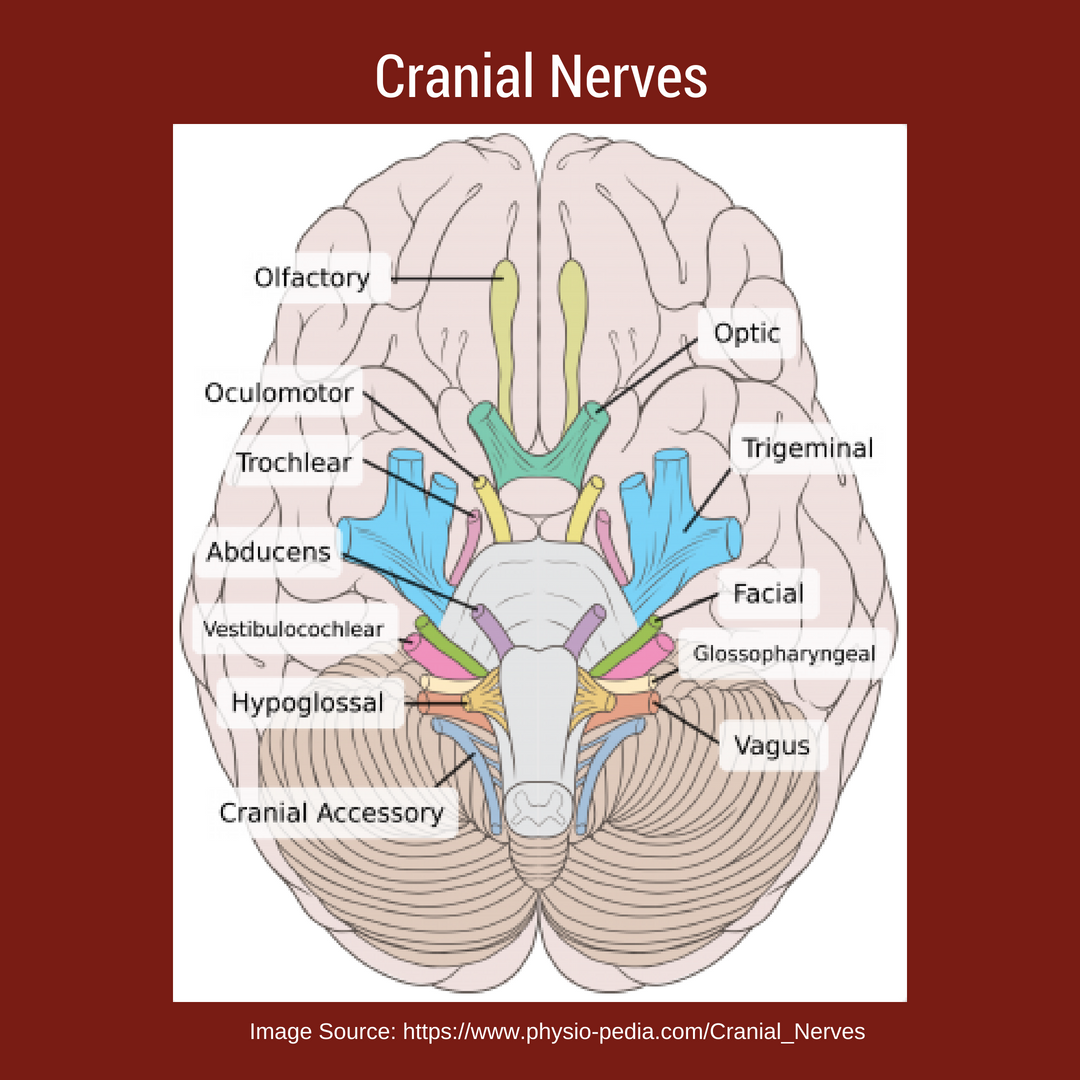
Topic #3: Cranial NervesWhile TSPT blog has a few posts on the cranial nerves, I have referred to our friends over at physiopedia for more in depth information. There will be test questions on the cranial so you must know each one and their function. "There are 12 pairs of cranial nerves and they are numbered according to their position of where they originate in the inferior surface of the brain...The names of the cranial nerves sometimes correspond with their individual function. The cranial nerves are comprised of axons that are either sensory, motor or both." [Reference: Cranial Nerves]. Watch the video below to learn more!
Best of luck on your final weeks studying for the NPTE! Jim Heafner PT, DPT, OCS
|

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|
 RSS Feed
RSS Feed