
|
|
|
|
As many of you know, we recently launched a Home Exercise Portion to our website. They consist of many exercises that we prescribe and programs like VHI don't contain. I wanted to highlight one exercise today, the Quad Rock Back, because of all of uses for it. The exercise is a staple of the Shirley Sahrmann philosophy. While it is listed under the "Low Back" section, it is often prescribed for cervical, shoulder, and hip patients as well. We will break down how the exercise can be used for each region.
As described in the video, when this exercise is performed for cervical patients, often the head begins to extend or flex while rocking back. This is a result of abnormal movement and compensatory patterns in the cervical spine. For cervical spine patients, we encourage a chin tuck so that no neck movement occurs during the rocking.
There are many reasons why I like to give this exercise to shoulder and hip patients, one being joint compression. We are taught in our manual therapy classes that joint compression can be beneficial for healing; it also can help mobilize the posterior capsule. It also helps mimic the developmental patterns of weight bearing on the upper extremities, and thus is a critical part of rehabilitation. Additionally, the quad rock back exercise can be use to help normalize scapulohumeral movement patterns and avoid any compensatory activity. While performing the exercise, the movement can be completed by actively flexing the hips, instead of pushing away with the UE's. This allows the shoulder to move in a more normal pattern. Similarly, the exercise can help with unwanted hip musculature activity. By reversing the directions (instructing the patient to push with the hands and not actively flex the hips), the patient can decrease abnormal femoral head sliding and thus compete hip flexion less painfully. The exercise can be used both for treating and assessing and low back dysfunctions, and not just because it is one of the more comfortable positions for low back pain. If you take your patient into quadruped and have them rock back, pay attention to the pelvis, hips, and low back. You may note a deviation to one side, suggesting increased muscle activity, stiffness, or movement patterns. Often you will note premature lumbar flexion compared to end-range hip flexion. This is secondary to all the sitting we do throughout the day - our lumbar spine becomes more flexible compared to the hip! By encouraging the patient to maintain a stable lumbar spine while rocking back (this can be done by placing a stick across the low back - if it falls off, we know there has been abnormal movement). This teaches our patients to isolate hip movement from back movement. While I may not subscribe to all of Sahrmann's theories on movement impairment syndromes, especially in the acute phase, I do appreciate the focus she places on changing compensatory patterns with her exercises. Many of these patterns stem from abnormal postures or repetitive tasks that we perform throughout our daily lives. The rehab focuses on resisting any changes in movement that occur as a result. I have found that I get better results with incorporating repeated motions into my treatment, but I continued to use Sahrmann exercises to try and retrain movement afterwords. -Chris
1 Comment
In the video below, Kelly Starrett discusses how sitting throughout the day places the hip joint in a poor position for normal daily movements. In the video he discusses how prolonged sitting places the psoas muscle in a short, contracted position. As an individual attempts to stand from this position, he/she hyper-extends the lumbar spine. Biomechanically, a tight psoas and shortened lumbar paraspinals draw the pelvis into an anterior pelvic tilt and the lumbar vertebrae into extension. Be aware: the chest may appear upright- giving the impression of natural movement,- but a closer look at the L-spine reveals movement beyond the neutral range. The problem with sitting exists beyond the chair as well. Normal standing posture requires little muscular action to maintain an upright position. In the presence of a hip flexor contracture due to prolonged sitting, forces are placed anteriorly across the hip requiring the hip extensors to counteract the force. Increased muscular action and metabolic cost creates the desire to sit, perpetuating the circumstance which initiated the hip flexion contracture (Neumann 2010).
The Student Physical Therapist Advice: Engage the Transversus abdominus (TrA) prior to moving from sitting to standing. The TrA provides a posterior pelvic tilt to counteract the force of the psoas muscle. Additionally a posterior tilt does not allow the lumbar paraspinals to contract as readily. With proper cueing, the gluteus maximus can then be engaged and stress will be taken off the low back. Enjoy the video- Jim References: Neumann, Donald. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 2nd edition. St. Louis, MO: Mosby Elsevier, 2010. 341-342. Print.  We are all guilty at one time or another of prescribing a hamstring stretch prematurely. You saw a patient bend forward to touch their toes and they abruptly stop short. This must be their hamstrings stopping their motion! Well unfortunately it is not that simple anymore. Modern literature tells us the reason they cannot touch their toes may be due to an array of possibilities: tight posterior chain muscles, adverse neural tensioning, or poor stability/motor control of the core musculature just to name a few. For the sake of this post we want to address hamstring tightness vs. adverse neural tension.
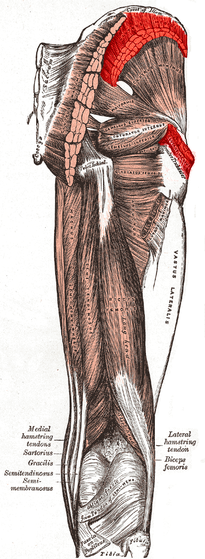
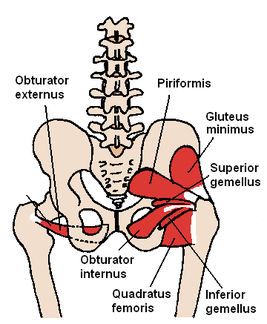
To begin this conversation, let's take that same patient above and place him/her in long sitting to reduce the effects of spinal loading. Now, postural demands are less than that in standing. We can focus specifically on muscle tightness vs. neural tension. The patient leans forward to touch their toes, but again nothing changes. We are no closer to finding our solution than we were in standing. Now, we bring the patient into supine, and the therapist performs a passive straight leg raise (PSLR). The patient cannot raise beyond 60 degrees of hip flexion. We still do not know, but we are getting close to the answer. Is it muscle tightness that is stopping this patient at 60 degrees or is the act of passively straightening the leg causing strain on the neural tissues. To answer this question, simply palpate the ASIS as you perform the PSLR. If you notice that hip flexion stops prior to movement at the ASIS, the answer is Neural Tension. If the ASIS begins to move prior to resistance, then hamstring tightness is the answer. Since the hamstrings attach to the Ischial Tuberosity, the body will naturally begin to posterior pelvic tilt once all the available range is taken up in the hamstring muscles. This posterior pelvic tilt will cause movement at the ASIS, letting you know the hamstring muscles have reached their end range. If no movement was noted at the ASIS, you can shift your hypothesis towards adverse neural tension. An additional component you can consider is the use of cervical flexion/extension to change the tension of the nerves and thus potentially alter SLR ROM. Just like any examination test, it is important to cluster your findings with other tests and measures. For example, if you suspect adverse neural tension, perform a SLUMP test as well. Additionally, always check side to side symmetry. 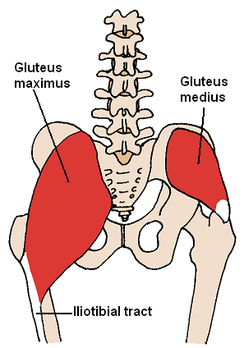 If you are familiar with Florence Kendall's method of Manual Muscle Testing (MMT), you are likely aware of the fact that she prefers to test muscle strength in a partially shortened position. When muscle length is in mid-range, it allows optimal cross-bridge linking, leading to a higher potential for force production. When muscles are over-extended or excessively shortened, the muscles lose that high frequency of cross-bridge linking. If you look at Kendall's MMT for the gluteus medius, you might see that she tries to emphasize the posterior fibers by having the patient on the side with the pelvis tilted forward and hip in extension, abduction, and lateral rotation. This is position completely shortens the muscle, thus potentially lower the validity of strength assessment. We have already discussed the use of evaluating hip abduction strength in a closed-chain position. Something else to consider is the fact that the gluteus medius is essential for pelvic stability throughout the entire stance phase of the gait cycle, not just mid-stance (where Kendall tests). Does it really matter if you have a level pelvis at midstance if you cannot keep your pelvis stable at heel strike? We have been presented another method for testing the gluteus medius in open-chain. Instead, place the lower extremity in hip abduction, lateral rotation, and flexion. The examiner then applies a flexion and adduction directed force. This position allows the muscle to not be completely shortened and tested in a functionally useful position. The position of flexion that is added can mimic heel strike in the gait cycle, making certain the muscle is strong enough to prevent pelvic drop as soon as stance begins.
 In the clinic, we often only have the length of the gym to analyze a patient's gait pattern. They patient may walk back and forth 2-3 times, giving you a total of 30 seconds to 1 minute to fully assess their pattern and recognize any deviations.
In this post from the Physioblogger, he discusses his Quick Gait Assessment. His assessment includes looking at the feet, hips, and trunk. He starts at the feet and works cephalad. Beginning at the feet, he assesses heel to toe progression and the amount of pronation/supination. Next at the hips, he analyzes frontal plane motion and the amount of pelvic sway. Finally in the thoracic region, quick notes are made on the amount of arm swing and trunk stiffness. Important points: -No diagnosis is made during the gait assessment. Formulating hypotheses as to why a deviation is present is fine, but do not make definitive judgements as to why deviations are occurring. It is simply an observation. -Always remember a patient's injury, mechanism, lifestyle. What structures are involved? How can this injury/ their lifestyle impact the gait cycle? -If possible, videotape your patients! Watch their gait patterns after they are gone. Take a few notes, perform the appropriate tests and measure, and act accordingly! Everyone has a different system they use for their quick gait assessment. Having a consistent method and practicing that method is important to your success as a therapist. Remember, we are movement analysis specialists.  If you feel like we having been referencing The Gait Guys a lot recently... it is because we have! They have put out a few great segments recently including this 2 part series on the Power of Observation. As clinical novices, we often do not have enough opportunities to see pathological gait patterns and conditions. As former students, almost of our lab "patients" were healthy classmates. While those experiences were rewarding, they were far from a real situation.
In this series, Shawn and Ivo dissect a triathlete's gait pattern. The patient presents with chronic low back pain, but has impairments throughout the entire lower chain. One interesting impairment they discuss is a "clenched fist on the L," which they attribute to flexor dominance and related to decreased arm swing and proprioceptive deficits. Their explanation: the proprioceptive system feeds the cerebellum. The cerebellum helps fire axial extensors. Because proprioception is limited in this athlete, the patient is naturally drawn into a flexor dominant position. Check out the entire post to gain more gems like this one! Because the gait guys use a Tumblr format, you may have to scroll down to June 25 and June 26. Enjoy!
This is a good, quick 7-minute TED Talk given by the orthopaedic surgeon, Dr. Kevin Stone. He presents several interesting concepts and innovative strategies about the future of joint replacements. This might not be something you see in your clinical practice today, but as science continues to improve Dr. Stone's biological approach to joint replacements could be something you see on a more regular basis. Check it out! 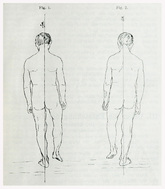 We are all aware of the standard MMT for the gluteus medius in sidelying, but how well does this assessment transition to functional activities like walking? A sign we occasionally see is the Trendelenburg sign. This may consist of the uncompensated type (contralateral pelvic drop) or compensated type (ipsilateral trunk lean). Why not use Trendelenberg as a test as well? The Gait Guys had a recent post where they review this functional method of assessing gluteus medius strength. They include the various compensation methods to watch out for along with potential causes for the impairment. Check it out!
|

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|


 RSS Feed
RSS Feed