
|
|
|
|
Your athlete comes into see you and has bruising and pain around the lateral ankle, extending down to the foot. He reports that he was at basketball practice and turned his ankle pretty hard. He has a history of lateral ankle sprains and presents with increased swelling consistent with a lateral ankle sprain. Yet, he complains of pain along the lateral aspect of his foot and some pain on the plantar side. The above scenario is something I have seen many times. Just last year I had a NBA draft prospect that sprained his ankle during a draft workout but was not getting better and had trouble walking. By the time I saw him he was 6 weeks from date of injury and struggling to understand why his ankle sprain wasn't better. There was a slight prominence on the plantar side of his foot about where the cuboid was. He had lots of pain with walking and weight bearing with pinpoint pain around the cuboid. I performed a cuboid whip and he immediately had relief of pain. Cuboid syndrome is an often overlooked diagnosis with lateral ankle sprains and lateral foot pain. Cuboid whips are a very effective treatment for these type of injuries. Signs of cuboid syndrome often go unnoticed because of similarity to ankle sprains. Some of the more common signs include:
Learning to effectively treat ankle sprains and cuboid syndrome with manual therapy can be very beneficial. Check out the video below to learn how to perform some of mobilizations and manipulations of the foot! Learn how to perform some of the most beneficial mobilizations and manipulations of the mid-foot/forefoot Dr. Brian Schwabe, PT, DPT, SCS, COMT, CSCS Board Certified Sports Physical Therapist Learn more at Insider Access
2 Comments
July is here! This means that we are nearing the next National Physical Therapy Examination (NPTE) that is offered quarterly (July 24-25). After going to graduate school for three years to become Doctors of Physical Therapy, your ability to practice is determined by the NPTE. While the purpose of physical therapy school is to prepare clinicians to safely and effectively rehabilitate patients, the direction of school is developed to prepare students to pass the NPTE. Even with three years of schooling, the examination can be intimidating due to its length and significance. In this article, I will review various study methods and recommendations for the examination.  ResourcesThere are many different resources available to make studying for the examination a little less frightening. For starters, the primary prep books include Scorebuilders and TherapyEd. Each of these texts are updated annually to stay in line with the NPTE. They come with overall content summaries (Scorebuilders with various charts is easier on the eyes and TherapyEd is more outline based) and sample tests at the end of the book. The content summaries, while useful, are not typically sufficient by themselves. It is recommended that you take each topic in the book with which you are unfamiliar and expand upon it with either textbooks or notes from school. The most useful component of the books is the sample examinations and answers. These examinations and answer explanations provide reasoning as to why certain answers are viewed as correct and others are "not as correct" (it is essential to remember that the exam often looks for the best answer available, not necessarily the true best answer). The exams will also give you an idea of how prepared you are overall for the NPTE and which specific areas you are deficient (there is an item analysis and breakdown after you complete each sample test). Both Scorebuilders and TherapyEd exam questions tend to be harder than the NPTE (the PEAT questions are most similar to the NPTE), but TherapyEd has the hardest questions. Because of this, I personally preferred TherapyEd as I like to be over-prepared for exams (I like to approach a difficult test and feel that it ends up being easy by comparison). There are several supplemental resources available as well. Both Scorebuilders and TherapyEd offer flashcards as a studying tool. If you are a flashcard user typically with studying, these may be useful. These companies also offer study prep courses that can be attended in-person. I attended the TherapyEd course, which while useful for understanding overall components of the exam, did not help in understanding actual content (that studying is left up to the individual). Finally, there are other companies that offer online prep courses and mentoring, such as PT Final Exam. Often these courses provide a timeline for studying the content, regular sample exams and feedback on areas to improve and methods for studying. Whatever resources may be best for you likely depend on your studying habits. Content FocusAs a general rule, it is recommended that the primary studying focus on the "Big 3." Somewhere around 60-70% of the NPTE questions will be based off the Musculoskeletal, Neuromuscular, and Cardiopulmonary subjects. They may include interventions, foundational information, examination or any other subtopics, but those three subjects comprise the majority of the test. With that said, studying should focus on these areas and add in the other subjects (i.e. modalities, ethics, etc.) as you feel more confident with the major topics. Should you feel confident in any specific area, you can spend less time studying that subject. I felt much more knowledgeable with the Musculoskeletal content, so I focused on the other two. The item analysis from the practice exams is perfect for finding those areas of weakness and strength, so it may be beneficial to take a baseline practice test and then at various intervals so you can continue adjusting your studying focus as you move closer to the NPTE. If you are short on studying time, focus primarily on the "Big 3" and touch up with the remaining areas of weakness.  Study TacticsGenerally, I recommend using the study tactics that you found successful when going through school. If you did well studying in groups, study in groups. If you did well with using flashcards, use flashcards. If you took longer to study for an exam, start earlier. I recommend starting with a practice exam to establish your baseline strengths and weakness. From that point, make sure you make the "Big 3" strengths and then move onto the other areas. Use the test prep book as your foundation for studying. I recommend working your way through each section and expanding upon a specific diagnosis, intervention, etc. using your class notes or text books. When you go through the practice exams, not only do you want to see why certain answers are wrong and certain answers are correct, but keep a mental log of the type of questions that are asked. This may redirect how you have been assessing and studying each topic. Finally, I recommend setting a schedule to study the content with more time allotted for the larger areas and some time left over leading up to the exam for final review and "touch up." This will keep you on task and ensure you cover the necessary material. While preparing for the NPTE, it is essential to take time to exercise, reflect/meditate, and relax. Whatever you use for stress relief will only facilitate your studying. The evening before the exam, I recommend taking it easy (don't cram!) and do something enjoyable: go out to eat with some friends, watch a movie, distract yourself from the exam and allow mind to rest as it prepares for the big day. If you have any other specific questions about how to prepare for the NPTE, feel free to reach out to us as we would be more than happy to help you make that transition to a licensed physical therapist! -Dr. Chris Fox, PT, DPT, OCS Interested in Learning More?Check out our Cervical and Lumbar Courses (on a 50% SALE until 7/5/18)
Understanding hindfoot mechanics is tough! Unlike the shoulder or knee joint, the multiple joints in the foot and ankle complex do not follow standard concave/convex arthrokinematic patterns. Additionally, the complex mechanics change whether or not the individual is in an open or closed kinetic chain. For example, movement at the subtalar joint consists of the triplanar motions of pronation and supination.
Talocrural Joint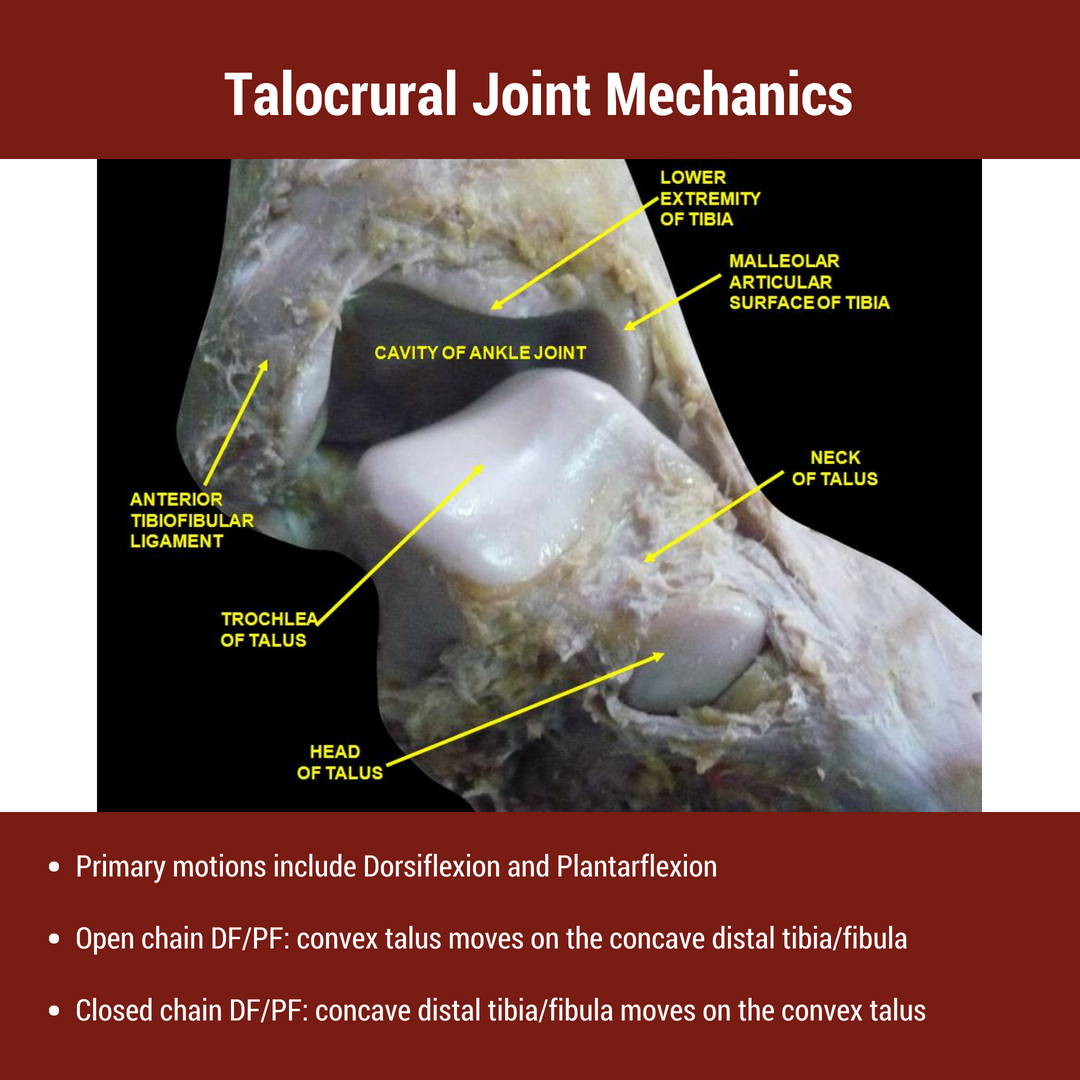 The foot and ankle consists of 26 bones and 100 distinct muscles, ligaments, and tendons. The rearfoot (a.k.a hindfoot) primarily refers to the talus and calcaneus bones of the foot. The talus articulates with FOUR seperate bones- the tibia, fibula, calcaneus, and navicular bones. The superior articulation between the talus and tibia/fibula is known as the talocrural joint. The talocrural joint is a uniaxial synovial joint connecting the distal tibia to the talus. While many people view the talocrural joint as only a hinge joint, others authors argue that it is more complex due to the composite internal and external rotation that occurs during dorsiflexion and plantarflexion respectively. For the purpose of this post, the primary movements at the talocrural joint are plantarflexion and dorsiflexion. The average individual has approximately 15-20 degrees of dorsiflexion and 50 degrees of plantarflexion. These motions are often limited due to inadequate stress and load through the joint. Subtalar Joint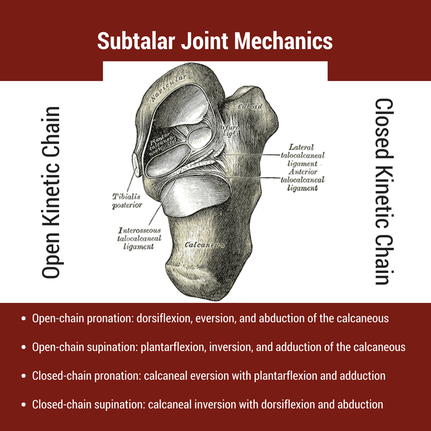 The subtalar joint (a.k.a. talocalcaneal joint) is comprised of the talus and calcaneus bones. As described in the introduction, the primary motion at the subtalar joint is pronation and supination. However, pronation and supination are not simple movements- both consist of 3 distinct movements, which changes depending on the foot's location to the ground. During ambulation, closed chain pronation must occur during the stance phase. This motion consists of calcaneal eversion combined with talus adduction and plantarflexion. This is described nicely in a post from the Gait Guys, "In a perfect biomechanical world, shortly following initial contact with the ground, the calcaneus should evert 4-8 degrees, largely because the body of the calcaneus is lateral to the longitudinal axis of the tibia. This results in plantar flexion, adduction and eversion of the talus on the calcaneus, as it slides anteriorly. At this point, there should be dorsiflexion of the transverse tarsal (calcaneo-cuboid and talo-navicular joints). Due to the tight fit of the ankle mortise and its unique shape, the tibial rotates internally (medially). This translates up the kinetic chain and causes internal rotation of the femur, which causes subsequent nutation of the pelvis and extension of the lumbar spine. [Citation: Gait Guys]" The subtalar joint must have adequate mobility to allow for proper structure of the arch. When motion is restricted, mobility issues often arise in the midfoot or at the talocrural joint as a compensatory strategy (see treatment video below).
Hindfoot Mobility: Foot Assessment and InterventionsThe human body must be able to adapt to all types of surfaces- hard, soft, even, and uneven. For this reason, we cannot solely look at one joint or one motion. As human beings we must perform all motions in harmony. While each of these movements may not have an impact on one's pain, understanding the kinematics can help with clinical reasoning and decision making! In the video below, I discuss variations in rearfoot posture, the impact on foot mobility, and how I incorporate these variations into my treatment. [this video comes from our insider access library!] Interested in Learning More? |
 |  |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages
Insider Access pages


We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!
Archives
July 2019
June 2019
May 2019
March 2019
February 2019
January 2019
December 2018
November 2018
October 2018
September 2018
August 2018
July 2018
June 2018
May 2018
April 2018
March 2018
February 2018
January 2018
December 2017
November 2017
October 2017
September 2017
August 2017
July 2017
June 2017
May 2017
April 2017
March 2017
February 2017
January 2017
December 2016
November 2016
October 2016
September 2016
August 2016
July 2016
June 2016
May 2016
April 2016
March 2016
February 2016
January 2016
December 2015
November 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
February 2015
January 2015
December 2014
November 2014
October 2014
September 2014
August 2014
July 2014
June 2014
May 2014
April 2014
March 2014
February 2014
January 2014
December 2013
November 2013
October 2013
September 2013
August 2013
July 2013
June 2013
May 2013
April 2013
March 2013
February 2013
January 2013
December 2012
November 2012
October 2012
September 2012
August 2012
Categories
All
Chest
Core Muscle
Elbow
Foot
Foot And Ankle
Hip
Knee
Manual Therapy
Modalities
Motivation
Neck
Neural Tension
Other
Research
Research Article
Shoulder
Sij
Spine
Sports
Therapeutic Exercise
 RSS Feed
RSS Feed