
|
|
|
 Low back pain is one of the most prevalent “dx” physical therapists see across the board. So how does low back pain management change with athletes? In some ways it’s exactly the same and others completely different. The important thing is to pay attention to the big picture stuff so you don’t miss a major injury. Let’s talk about some of the major things we want to look out for and consider with the low back pain athlete. First of all, low back pain is not a normal finding. There is a reason the athlete is experiencing low back pain. For example, when I have a football lineman or gymnast come to me with low back pain my PT senses are automatically heightened. Why? Because these particular sports and positions are more predisposed to having a potential spondylolysis or spondylolisthesis. The reason being is the repetitive hyperextension and vertical loading required in these sports/positions. Therefore, part of my screening process is determining if I need to get these athletes imaging. From there, the management of these athletes with pars defects depend on the degree of slippage. For example, if an athlete has a lower grade slippage than often there is some period of activity restriction until pain subsides and then most importantly a gradual reloading with activity. Another diagnosis often seen is disc issues. These are more common than one would think and can be another injury that takes an athlete out for some time depending on the severity. Athletes that undergo more axial loading, flexion and rotation in addition to collision sports are often in the higher rate of athletes with lumbar disc herniations. One clinical pearl to offer is that sometimes when there is nerve involvement, the motor function is more affected than the sensory function. Therefore, just because an athlete doesn’t complain of the “common” tingling or numbness in the leg, doesn’t mean you should skip a myotomal exam. Return to sport following a low back injury in the athlete can be another challenge. While there is no “gold standard” return to sport testing for low back pain, plenty of data exists that athletes can return at a very high level following a low back injury (ex: Tiger Woods, Rob Gronkowski). Instead of the common algorithm like the knee has with hop tests (etc), the lower back is a little more multifactorial. However, similar principles apply. Return the athlete to his/her baseline function, clean up movement abnormalities, re-establish strength levels, and have a gradual return to sport with controlled to uncontrolled practices in the respective sport. There is no one way and we should not make it one way. Instead, understanding the needs analysis of the sport, position, and the athlete’s previous level of function should be our goal. Low back pain in athletes can be a challenging case to manage. While it starts with a very solid assessment, understanding the biomechanics and positional demands of the respective sport will guide your interventions and eventual return to sport. Make sure you understand each sport and position carefully. For more information on return to sport considerations in the athlete and specific progressions and regressions, check out our Insider Access. Dr. Brian Schwabe, PT, DPT, SCS, COMT, CSCS Board Certified Sports Physical Therapist Frustrated with tough patient cases? Can't afford a sports or orthopedic residency? Want more skills to advance your career? Check out our TSPT official courses! |
 |  |
2 Comments
If you are a new graduate, treating acute low back pain can be frightening. Often times, a patient arrives in agonizing pain with a limited ability to do any movement. In these moments, your standard examination is dismantled. The natural default mode is to start performing every lumbar spine test and measure you learned in Physical Therapy school. In these moments, you gather information without considering ‘why’ you chose to perform the test and 'how' the outcome would impact your overall plan of care. It is in these moments that you realize that the special tests are not very special. So what happens next!? The answer is a better, more efficient evaluation from the start!
Key Lumbar Examination Points
- Minimal positional changes for the patient. It is inefficient to have the patient constantly rolling over, standing, and sitting. A patient in high levels of pain will not be able to tolerate multiple positional changes.
- Perform pain provocation testing last in each position. For example, if a patient states that bending forward increases their symptoms, perform lumbar flexion active range of motion last. Pain will cloud the results of your physical exam.
- Examiner must assess regional joints, muscles, and nervous system tissue. The body is a single kinetic chain. Movement at one joint increases the demands on local tissue. For example, when someone performs shoulder flexion, movement occurs in the thoracic spine, rib cage, acromioclavicular joint and more. If one of those areas is dysfunctional, it can be the source of pain. Each examination needs to evaluate each source of a patient’s symptoms.
Lumbar Examination: Efficiency and Reliability
A good clinician will follow the same general steps when performing any Physical Therapy Evaluation. These tests and measures are performed in a systematic, reproducible manner. While the clinician may add or remove testing as needed, the general framework for formulating their diagnosis is consistent. This consistency allows for efficiency and reproducibility. For example, in the lumbar evaluation the examiner assesses the function of the core muscles in supine; however this should only be completed after a thorough examination of the functional testing of the core in standing. It would not be an efficient use of time to take an acute low back pain patient from standing, to supine, back to standing, to prone. The entire session would be disrupted with positional changes. Additionally, the goal of any physical therapy session is to maximize the patient's functional ability so we must assess function first.
What is clinical efficiency?
 | AT IT'S CORE, CLINICAL EFFICIENCY IS ARRIVING AT THE CORRECT PHYSICAL THERAPY DIAGNOSIS AND DETERMINING THE APPROPRIATE PLAN OF CARE WITHOUT PERFORMING UNNECESSARY TESTS AND MEASURES. |
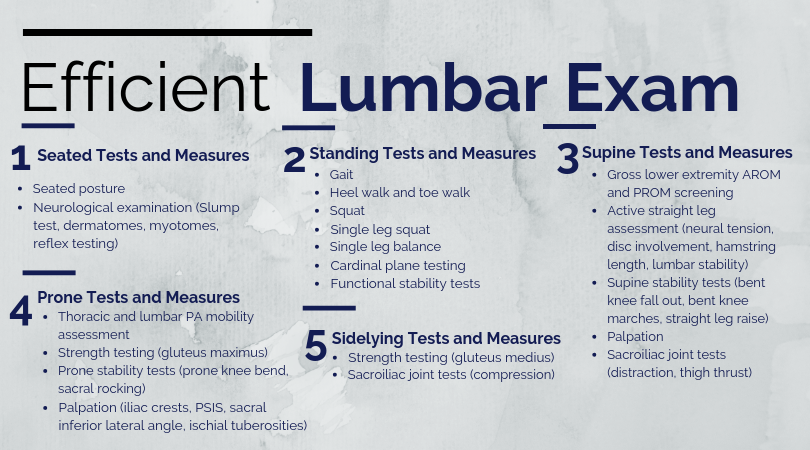
Lumbar Examination Sequence
Lumbar Interventions: Typical Day 1 Treatment and More
Similar to my shoulder evaluation post, my Day 1 lumbar interventions heavily focus on desensitizing the painful tissue through graded tissue exposure. Additionally, I spend a significant amount of time educating the patient on pain science.
Below are 3 common exercises I give patients on the first day
Hand Heel Rocks

General Cues
- Position yourself so that your hands are directly under your shoulders and knees are directly under your hips
- Rock backwards as far as you can before your lower back starts to round
- Make sure that your head does not start to look up or drop down and that your lower back does not round during the exercise
Supine Hip External Rotation

General Cues
- From a hooklying position, bring one leg over the top of the other
- Use your hands to press your thigh further into hip rotation
- Engage the lower abdominals to minimize movement from the low back (this movement is not bad, but just not the purpose of this exercise)
Prone Press-ups

General Cues
- From your stomach, use your hands to press up into back extension
- Relax your glutes and low back to sink further into the movement
Bonus: Foam Roller Thoracic Extensions

General Cues
- Place the foam roller across your middle back
- Arch over the foam roller while keeping the core engaged (this minimizes the movement across the low back-- important if they are in pain)
There are no single set of exercises for every patient. Their individualized pain triggers and tolerance to exercise will heavily dictate what they can do!
Jim Heafner PT, DPT, OCS
Jim Heafner PT, DPT, OCS
Check out our Insider Access Page!
| Learn from residency-trained, board-certified orthopaedic and sports physical therapists. With Insider Access, you gain access to advanced manual assessment and treatment techniques, exercise progressions, sports specific content, and more. Our goal is to facilitate your clinical and professional growth! |  |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages
Insider Access pages


We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!
Archives
July 2019
June 2019
May 2019
March 2019
February 2019
January 2019
December 2018
November 2018
October 2018
September 2018
August 2018
July 2018
June 2018
May 2018
April 2018
March 2018
February 2018
January 2018
December 2017
November 2017
October 2017
September 2017
August 2017
July 2017
June 2017
May 2017
April 2017
March 2017
February 2017
January 2017
December 2016
November 2016
October 2016
September 2016
August 2016
July 2016
June 2016
May 2016
April 2016
March 2016
February 2016
January 2016
December 2015
November 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
February 2015
January 2015
December 2014
November 2014
October 2014
September 2014
August 2014
July 2014
June 2014
May 2014
April 2014
March 2014
February 2014
January 2014
December 2013
November 2013
October 2013
September 2013
August 2013
July 2013
June 2013
May 2013
April 2013
March 2013
February 2013
January 2013
December 2012
November 2012
October 2012
September 2012
August 2012
Categories
All
Chest
Core Muscle
Elbow
Foot
Foot And Ankle
Hip
Knee
Manual Therapy
Modalities
Motivation
Neck
Neural Tension
Other
Research
Research Article
Shoulder
Sij
Spine
Sports
Therapeutic Exercise
 RSS Feed
RSS Feed