
|
|
|
 With the development of pain science research, we regularly are seeing studies come out the show a lack of correlation between pathological findings on imaging and pain. Arthritis can start as early in the teenage years. Bulging discs and spinal stenosis are another sign of aging. One is almost abnormal for not having these findings. The only types of diagnoses that seem to benefit from imaging include fractures, infections, tethered cord syndrome, tumors and similar ones. As I've mentioned recently, I've been reading the McKenzie texts to build a better understanding of the foundation of repeated motions. One of the diagnoses that many believe indicates we should not perform repeated extensions is spondylolisthesis. For those of you unfamiliar with the pathology, it typically represents a fracture of the pars interarticularis and slippage of the vertebra relative to the adjacent ones. The theory is that repeated forceful lumbar extension is the cause of spondylolisthesis via repetitive microtrauama, as this is frequently seen in gymnasts, volleyball players, dancers, and more. In the book, spondylolisthesis was actually not presented as a contraindicated. According to Spratt et al 1993, those with spondylolistheses have actually been shown to have an excellent response to repeated lumbar extensions. Now this can be interpreted in a couple different ways. It's possible people had an asymptomatic spondylolisthesis while also presenting with a symptomatic "disc injury" (excuse the pathological explanation). More appropriately, the patient may still have an extension directional preference, meaning they improve with repeated extensions. 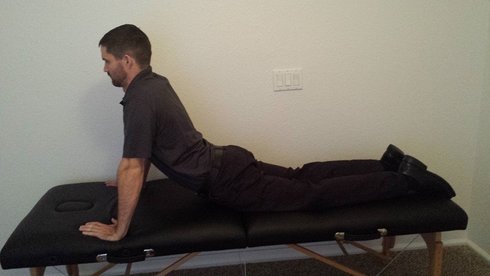 Given this information, it's hard to know if we should associate spondylolistheses with repetitive microtrauma and "true pathology" or if it is simply another sign of aging. In my opinion, we should take any potential imaging findings and see if they connect with our clinical examination to determine if we should consider if a potential spondylolisthesis is pertinent to our patient's presentation. Simply because a patient has a spondylolisthesis doesn't necessarily mean that the specific pain episode they are presenting with doesn't have a directional preference of extension. Be sure to look at overall mobility deficits to decide which direction is most likely to respond. -Dr. Chris Fox, PT, DPT, OCS Reference: Spratt KF1, Weinstein JN, Lehmann TR, Woody J, Sayre H. Efficacy of flexion and extension treatments incorporating braces for low-back pain patients with retrodisplacement, spondylolisthesis, or normal sagittal translation. Spine (Phila Pa 1976). 1993 Oct 1;18(13):1839-49.
1 Comment
Nick
10/4/2016 05:50:19 pm
Spratt's intervention was more accurately sustained extension rather than repeated extension, but I reckon your point still stands. Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|

 RSS Feed
RSS Feed