
|
|
|
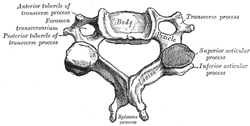 Individuals with mechanical neck pain often have pain and a loss of mobility in the upper cervical spine, specifically at the atlanto-axial (C1-C2) joint. This joint is primarily responsible for cervical rotation, but also contributes to small amounts of flexion and extension. Arthrokinematically, during left rotation, the left facet of the atlas(C1) glides posterior on the axis (C2) & the right facet of the atlas glides anterior. During flexion, the facet of the atlas glides anterior and rolls posterior in relation to the axis. The opposite happens with extension. There are 2 different theories as to how to assess the mobility of C1-C2. At Harris Health, I learned to maximally side bend the head, followed by opposite rotation. For example to assess C1-C2 rotation to the left, maximally side bend the head to the right, followed by maximal rotation to the left. The maximal side bend "locks out" the lower cervical vertebrae allowing for motion only at the C1-C2 junction. The other method to assess C1-C2, which I learned in PT school at St. Louis University, is the flexion- rotation test. To perform this test, maximally flex the cervical spine followed by maximal rotation either left or right. Flexion is thought to lock out all vertebrae below allowing for rotation at C1-C2 only. The difficulty with the flexion-rotation test is maintaining flexion while maximally rotating the upper cervical spine. From my experience, there is a tendency to lose upper cervical flexion.
In the residency, I learned that the flexion-rotation test assesses C1-C3. One can then differenciate C1-C2 restrictions from C2-C3 restrictions by first performing the side bend rotation test first, then performing the flexion rotation test. If greater rotation is achieved during the flexion-rotation test vs. the sidebend then rotation, it can be assumed the dysfunction is greater at C1-C2 joint.
It is important to understand that different programs teach different methods of assessment. One method is not better than the next as long as there is sound reasoning behind your decision making. Does anyone else assess C1-C2 differently or have preference with one method over the other? Let us know! -Jim Thank you to the Harris Health Orthopedic Residency for letting me use images from their Cervicothoracic Module Workbook.
5 Comments
Kenny Carlton
4/16/2014 06:39:36 am
Just wanted to let you know you have C1 and C2 mixed up here. "Arthrokinematically, during left rotation, the left facet of the atlas (C2) glides posterior on the axis (C1)" Otherwise, nice article.
James Heafner
4/16/2014 08:40:41 am
Kenny,
Griffin Lee
4/25/2014 09:44:23 am
Great post. I have learned and generally use both of these assessment techniques. I feel that it is good to know how to perform and use both so that you have multiple options to assess C1-2 in case you are unable to accurately assess it in instances like you mention where you may not be able to maintain upper cervical flexion or maybe you lose sidebend when you add the rotation component.
Justine
8/9/2014 11:44:40 am
so.. I'm confused. This guy Kenny says C1 is "axis" and C2 is "atlas". that is incorrect.
akash
12/11/2015 01:41:16 pm
Hi, I have upper cervical instability from an alar (possibly transverse as well ligament injury to my left side). I suspect it tore and healed weak. Fell with my head rotated. Is there a way that it can be strengthened? My PT is unaware of any method and would appreciate any tips or guidance (and needless to say, so would I). Any help would be welcome!! Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|


 RSS Feed
RSS Feed