
|
|
|
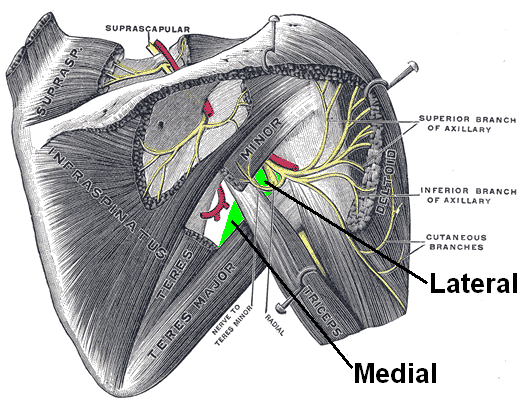
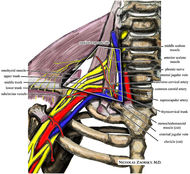 One of the greatest risks following an anterior shoulder dislocation is damage to the neurovascular structures which surround the glenohumeral joint. Due to their anatomical location, certain nerves are at a higher risk of injury than others following a dislocation. Additionally the position and displacement of the arm during the injury is another factor to consider. For example, "a fall with the arm in full abduction and internal rotation causes major tension on all nerves and cords." The Visser et al article also mentioned that concurrent fractures and the presence of a hematoma increasead the risk of nerve damage. Nerves that are at the greatest risk of injury include the axillary, suprascapular, and musculocataneous nerves. Throughout the literature, authors have found that the axillary nerve is most frequently and severely damaged (Visser). The axillary nerve originates from the upper trunk, posterior cord of the brachial plexus carrying nerve fibers from C5-C6. It courses around the surgical neck of the humerus before entering the quadrilateral space (see middle picture below to review the space boundaries). The nerve gives off muscular branches to the deltoid, teres minor, and long head of the triceps brachii. Due to the close association to the surgical neck, the axillary nerve is often compromised during an anterior-inferior shoulder dislocation. A study by Visser et al found that 42% of their 77 patients had axillary nerve insult following a low-velocity trauma anterior shoulder dislocation.
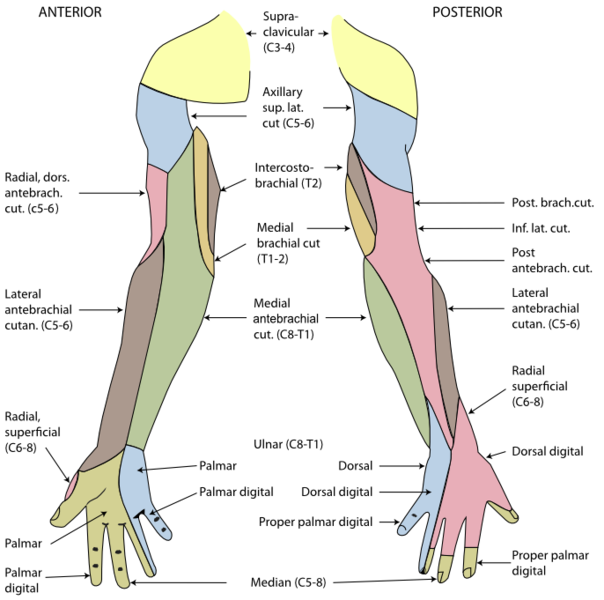
Due to the high incidence of nerve related injuries, a complete neurovascular examination is warranted following a shoulder dislocation. This examination should include MMT of the shoulder and arm musculature, palpating for the brachial pulse, and examining sensation of the arm. When assessing for axillary nerve damage in particular, a clinician should look for muscle atrophy of the teres minor and deltoid muscles. One should suspect weak flexion, abduction, and external rotation of the shoulder. Observation and palpation would reveal a flat shoulder deformity due to deltoid atrophy. Additionally, they will have a lose of sensation over the upper lateral arm around the deltoid region due to denervation of the superior lateral cutaneous nerve of the arm (see right picture above). -Jim References:
Visser, C. P. J., L. N. J. E. M. Coene, R. Brand, and D. L. J. Tavy. "The Incidence of Nerve Injury in Anterior Dislocation of the Shoulder and Its Influence on Functional Recovery." The Journal of Bone and Joint Surgery 81.4 (1999): 679-85. Web.
1 Comment
5/12/2014 08:51:40 pm
Chiropractic clinics, health care centers and pilates fitness institutes are nothing less than a boon for victims of lower back pains. Chiropractors, health care experts and pilates instructors avert back problems from getting deteriorated. Standing or sitting for a protracted period of time can lead to chronic pain. Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|

 RSS Feed
RSS Feed