
|
|
|
|
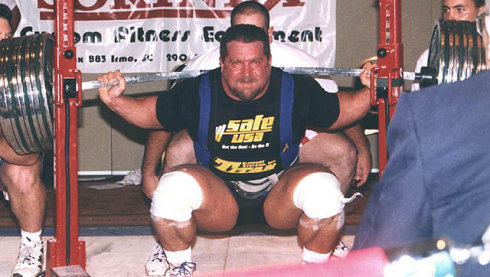
The Clinical Practice Guidelines (CPG) have been developed over the last decade with the goal of summarizing best practice methods for various orthopaedic diagnoses. While the utility of CPG's may be debatable, they do an excellent job providing a summary of the evidence for managing the specific conditions. With the hip being the focus of December, I am going to review what the evidence shows for examining a patient with hip osteoarthritis and the appropriate interventions. Before getting started, a quick reminder for the grading system for research: A (strong evidence), B (moderate evidence), C (weak evidence), F (expert opinion).  Diagnosis (A): These patients are over the age of 50 and exhibit the following presentation (A-Level Evidence): -Moderate anterior or lateral hip pain with weight-bearing -Morning stiffness less than 1 hour after waking -Hip IR ROM < 24 deg or IR and Flexion < 15 deg compared to nonpainful side -Increased hip pain associated with passive hip IR Outcome Measures for Activity Limitation and Participation Restriction (A): -WOMAC -HOOS -LEFS -HHS Activity Limitation/Performance Measures (A): -6 Minute Walk Test -30 Second Chair Stand -Stair Measure -TUG Test -Self-Paced Walk -Timed SLS -4 Square Step Test -Step Test Balance Measures (A): -TUG Test -Berg Balance Test -Timed SLS Test Physical Impairment Measures (A): -FABER Test -Hip PROM -Hip Strength Testing As you can see, there are quite a few very reliable methods of diagnosing Hip OA and then tracking progress in function, balance, performance and impairment. It is in no way necessary to perform all of the above tests and measures. What I recommend from these is to identify your patient's goals and determine what outcome measures and performance measures will best track said progress. It is good to be thorough with the impairment measures in order to track objective changes. Once the patient has been diagnosed with Hip OA, there are several interventions that have shown varying levels of support. Interventions: -Education (B): activity modification, exercise, joint unloading, weight-loss -Functional Gait and Balance Training (C): gait/balance training and use of assistive device -Manual Therapy (A): thrust/non-thrust manipulation and STM and coupled with exercise -Flexibility/Strengthening/Endurance Exercises (A) -Modalities (B): US to ant/lat/post hip and coupled with exercises and heat -Bracing (F): should only be tried if exercise/manual therapy fail -Weight Loss (C)
As you can see, the typical trend for PT continues with treatment for this diagnosis: manual therapy and exercise have high level evidence. While education has moderate evidence, it would be interesting to see the benefit of education that was more focused on pain science, graded exposure, and cognitive behavioral therapy. These topics are more pertinent today given the findings of pain science research, especially given how frequently people have "Hip OA" and don't have any pain. Additionally, it was surprising to see that ultrasound had moderate evidence. Even so, I would recommend more focus be placed on exercise, education and manual therapy for these patients. As a whole, I think that the development of CPG's will help to improve the standard of care. There is far too much varied care due to misdiagnosis. That being said, patients don't present "standardized" and we are moving away from pathoanatomical diagnoses as well. Hip osteoarthritis is so common in people that it is almost surprising that it even has its own CPG. There are so many factors that go into a patient's pain and disability experience: financial situation, relationship stress, past experiences, fear, and more. No two patients present the same. I recommend take the recommendations from the CPG into consideration, but don't hesitate to modify your plan of care based on the patient presentation. -Dr. Chris Fox, PT, DPT, OCS
1 Comment
3/3/2024 07:48:52 am
Businesses play a crucial role in the global economy, driving innovation, creating jobs, and shaping market trends. In the realm of online commerce, trust is paramount. One might wonder, Is eDreams legit This question reflects the growing importance of verifying the legitimacy of online businesses. As consumers navigate the digital marketplace, ensuring the credibility of platforms like eDreams becomes essential. The success of businesses hinges not only on their products or services but also on establishing and maintaining trust with their customers, underscoring the significance of transparency and reliability in the ever-evolving business landscape. Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|

 RSS Feed
RSS Feed