
|
|
|
|
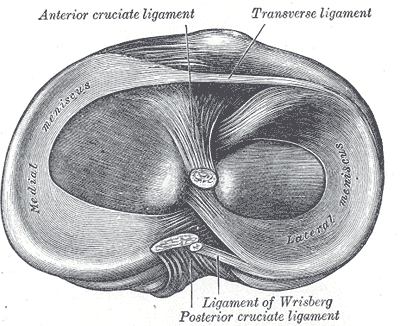
One knee injury that is frequently encountered in the clinic is the meniscus tear. The injury often presents after an acute incident with moderate swelling, pain and dysfunctional motion. Often, we hear about athletes needing surgery to treat these injuries (either meniscal repair or partial meniscectomy). Whether or not surgery is indicated is a different issue, but due to potential treatment options, it is beneficial to be aware of the tissue involved. How do we diagnose meniscal tears? There are a plethora of tests out there with varying diagnostic accuracy used for diagnosing meniscal tears. Probably the single test with best diagnostic accuracy is Thessaly's (Sn = .90; Sp = .98). Unfortunately, the test actually recreates the mechanism of injury and could potentially increase the tear, so it is not recommended. Instead, it is better to use a diagnostic cluster of tests by Lowery et al. The cluster utilizes 5 exam measures: Joint Line Tenderness, McMurray's, pain with knee flexion overpressure, pain with knee extension overpressure, and hx of joint locking/catching. With 4/5 positive tests, Sn = .17 and Sp = .96. With 5/5 positive tests, Sn = .11 and Sp = .98. While none of the clustered tests have great diagnostic accuracy by themselves, when utilized together, they become much more beneficial.
How do we treat meniscal tears? With recent research finding no difference between surgery and conservative treatment, as physical therapists we must be aware of providing our patients with the best opportunity to successfully complete rehabilitation. Early research has shown that cartilage and meniscus healing occurs with high repetition-low load training (Khan and Scott, 2009). That means thousands of repetitions at 15-20% 1RM in addition to treating any impairments present. I typically utilize either a recumbent bike or shuttle leg press. Should patients fail the conservative route, often they are sent on for a surgical option: meniscal repair in the younger population, partial meniscectomy in the middle-aged population, and total knee arthroplasty in the geriatric population. What does this mean to me? While I appreciate the evidence that supports conservative treatment compared to surgical, one of the often under-emphasized points is that meniscal tears often occur as natural aging, similar to how herniated disks naturally occur in the spine. Imaging is not as beneficial as we once thought, because most people will have some sort of degenerative findings. Personally, I focus on the primary impairments and address those. For example, in this patient population, I often find the patients present with either a lack of tibial IR or knee extension on the involved side. These patients frequently respond to repeated motions with improvements and pain and ROM. I also include IASTM and treatment of remaining impairments and movement patterns in addition to high rep-low load training. As always, an eclectic approach is best, but it doesn't hurt to include treatment for the suspected injured tissue. Whether or not it is true "healing" or has more of a pain-science desensitization effect, it may be effective. For this reason, I still advocate using special tests to determine potential tissue involvement. References: Khan and Scott. (2009) "Mechanotherapy: how physical therapists' prescription of exercise promotes tissue repair." British Journal of Sports Medicine. 2009; 43: 247-251. Web. 5 Dec. 2013. Lowery DJ, Farley TD, Wing DW, Sterett WI, Steadman JR. "A clinical composite score accurately detects meniscal pathology." Arthroscopy. Nov 2006; 22(11):1174-1179. Have you ever wanted to enroll in a residency but not have the time or ability to financially commit? Jim Heafner, PT, DPT, OCS, SFMA and Chris Fox, PT, DPT, OCS, SFMA from The Student Physical Therapist have partnered with Dana Tew, PT, DPT, OCS, FAAOMPT from Optim Physical Therapy to create a COMT program starting in October! The mission of the program is to develop the clinical reasoning and manual skills of the participants over the course of a year through a structure similar to a residency, but without the financial sacrifice and significant time commitment, The program will help you to prepare for the OCS, improve your outcomes, and qualify for Fellowship enrollment. Check out the program for more details at www.optimfellowship.com and let us know if you have any questions!
2 Comments
David
9/3/2015 06:34:18 pm
I like the specific prescription of 15-20% 1RM. I feel these parameters are not used enough in the clinic. What do you think the reasoning is for the presentation you described of lack of full extension and IR?
Hi David, Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|

 RSS Feed
RSS Feed