
|
|
|
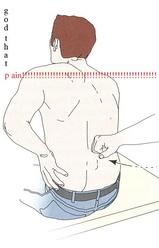 A few weeks back, I wrote a post about assessing for Lumbar Extension Rotation Syndrome (ERS) in low back pain patients. Since then I have received several comments from people wanting information regarding treatment options for this condition. Overview A typical patient presentation includes age >55 years old, chronic low back pain, and may be involved in a rotational sport (golf, tennis, etc). On physical examination, you will observe an exaggerated lumbar lordosis, paraspinal muscle asymmetry, excessive pelvic rotation during gait, and hinging during cardinal plane extension testing. They will often complain of unilateral lumbar pain that increases with extension and is relieved with non-weight bearing lumbar flexion. Generally a patient with ERS hyperextends their low back, which does not allow the gluts to fire properly. Treatment For the purposes of this post, I want to focus on core stability and lumbopelvic disassociation. I find that pure hip strengthening is not appropriate early on because the patient cannot adequately engage their gluteals without lumbar compensation. Since the patient has excessive lumbar lordosis and hinging during functional movements, addressing core stability is essential. Additionally, strengthening and motor control of the hip extensors and external rotators is important once the core has sufficient control. Manual therapy is performed on a patient-to-patient basis depending on individual impairments found during the physical examination. Since the patient is generally hypermobile at the hinging segment, they are hypomobilie cranially or caudally. Thoracic and lumbar mobilizations and manipulations are appropriate for the appropriate patient. Core Stability Assuming the patient has low irritability levels and good body awareness, I will usually begin TherEx by retraining the transversus abdominus (TrA) in supine. After the patient can maintain a neutral low back position, I will incorporate the bent knee fall out exercise using a blood pressure cuff for additional cueing. Many progressions of the blood pressure cuff are appropriate until the patient demonstrates good isolation of the TrA in supine. As the patient progresses, I take them through a progression of exercises in quadruped to ensure the patient can maintain a neutral low back posture in a gravity independent position. The progression includes isolated TrA contraction, TrA hand heel rocks (see below), and removing limbs from the table (alternating shoulder flexion, alternating hip extension, then birddog exercises). When the patient can demonstrate good control in quadruped, I address core control in spinal weight bearing. In standing, I have found using the wall as an external cue helps the patient 'find' their TrA. When appropriate, begin functional training in standing by incorporating mini-squats, lunges, and other upper and lower extremity disassociation exercises. Below is a progression of 3 common exercises I prescribe for ERS from supine to standing.
Please let me know if you have any questions or would like more information regarding treatment options of extension rotation syndrome. -Jim
3 Comments
Michael Carnell
1/17/2017 01:19:40 pm
What happens when you have tried everything? core, dry needling, chiro, pt, injections
Hi Michael,
Alec
9/4/2019 09:44:59 pm
Where can I get more information on the exercise protocol. I am dealing with this issue for quiet some time. Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|
 RSS Feed
RSS Feed