
|
|
|
|
Recently, I was mentoring with Optim Manual Therapy's online case study discussion and a case was presented where there was some confusion diagnosing peripheral neuropathy versus radiculopathy. Due to the similarity in presentation sometimes, I thought it would be good to go over some of the similarities between the two and how we can differentiate as well. I am going to focus on the upper quarter region, but the same concept will apply to the lower quarter as well. Below are a couple pictures of the peripheral nerve layouts and dermatomal patterns that I will reference throughout this post. 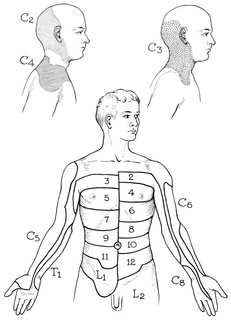 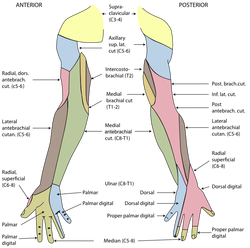 For starters, remember that both peripheral nerve lesions and radiculopathy are lower motor neuron lesions, so they can both present with corresponding weakness and hyporeflexia. Additionally, they can sometimes present with pain (or numbness/tingling) in similar regions. Think of the ulnar nerve and C8. Just because a patient has radiculopathy doesn't mean they have to have symptoms centrally/proximally as well. They both can present with symptoms along the ulnar border of the hand. Other regions have more distinct differences, for example, C7 tends to refer down the middle finger and no peripheral nerve typically presents in just that region. As you can tell, there are a lot of similarities, so how do we differentiate? There are several things to consider. An extremely useful assessment style is assessing muscle strength in muscles that have similar segmental input but different peripheral nerves. We'll go back to our C8 vs ulnar nerve example. Both are heavily innervated by the same segment and can present with symptoms in the same location. A key assessment feature is looking at the strength of Extensor Pollicis Longus. It is innervated by the radial nerve, but it's primary segmental input is C8. Should a patient have weakness here, we would be leaning more towards C8 radiculopathy. If it is strong, we would lean more towards ulnar neuropathy. The same concept can be applied to other areas. Another useful assessment is neural tensioning. Should the patient's exact symptom be reproduced with it, we likely would consider the nerve involvement; however, often radiculopathy does have a neural tension component to it, so it is not as helpful as we would like. Probably one of the best assessment techniques is using the cervical radiculopathy cluster developed by Wainner, et al: -Cervical Rotation <60 deg to involved side -(+) Median ULNT -(+) Cervical Distraction Test -(+) Spurling's Test This cluster has been shown to have high diagnostic accuracy for identifying those with cervical radiculopathy and is probably our best tool (3 positive: +LR = 6.1, 4 positive: +LR = 30.3). While one would think that pain with segmental mobility testing of the spine would be useful if pain is recreated, people can have symptoms in two locations as a result of Double Crush Syndrome or altered neurodynamics. Regardless, the most important thing is that we treat all impairments we are presented with. If the neck is stiff in someone with ulnar neuropathy, I'm still going to work on improving neck mobility. They key is that if there is research for a specific treatment for a specific diagnosis, it is important we try and identify these cases. Also, remember that there are other sources for symptoms other than peripheral nerves and radiculopathy. Patients can also present with symptoms in the exact same region due to trigger point referral patterns, local strains/sprains and more. Hopefully this will at least help with differentiating between two similar presentations. Check out the Insider Access Page for more information on this ! -Dr. Chris Fox, PT, DPT, OCS Reference: Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison S. "Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy." Spine (Phila Pa 1976) 2003 Jan 1.
8 Comments
Oleg
11/9/2017 12:06:28 pm
The topic is very well outlined in the book "Neurological differential diagnosis" by John Patten.
JR
7/10/2019 12:40:56 pm
This actually is very unclear.
Chris
7/10/2019 02:12:04 pm
Hello JR,
AR
8/18/2019 11:55:01 am
This is actually quite clear.
PJ
2/13/2021 03:24:37 pm
You begin by differentiating spinal nerves and peripheral nerves. Therein lies the confusion because Spinal nerves are peripheral nerves. All of nerves you mention here are in the PNS. It would help to first define what you mean by "peripheral" before using that term. Radiculopathy is a subset of Neuropathy and Neuropathy is a VERY general term. I think it is important to use terms that define the locus of nerve damage.
Priscilla Scott
4/11/2021 12:08:30 am
I have a genetic disorder Ehlers Danlos Syndrome, it’s a connective tissue disorder due to a mutation of the collagen gene. I have the vascular type and at age 46 I’ve lost the feeling in my fingers and toes , my knee right and left hip and have fractures from minor trauma due to osteoporosis & osteopenia... I’ve also been living with a dislocated coccyx bone that’s now pushing into my bowels ... causing issues eg biliary duct is inflamed and it gets a blockage occurring perhaps once or twice a month ... but my small local hospital won’t operate on me as they are too worried re my vascular Ed’s , so I sit uncomfortably and wait until they start giving me proper treatment eg magnesium and ketamine infusions for pain and also Vit c to help my immune system..., my stomach can’t absorb nutrients and it’s already shut down ... I can’t eat but I do drink water and take fluids ... there isn’t enough research into this illness which is a shame as many have it ... thanks 🙏🏽 2/14/2024 12:13:58 pm
I just had it EMG test done. It came back chronic ridicuradiculopathy and bilateral neuropathy for the VA without a EMG test done I get a 20% disability for right leg radiculopathy 20% for left leg radiculopathy. I’m not sure how they determined any kind of rating and how do I differentiate neuropathy from the radiculopathy or determine how severe my radiculopathy is Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|


 RSS Feed
RSS Feed