
|
|
|
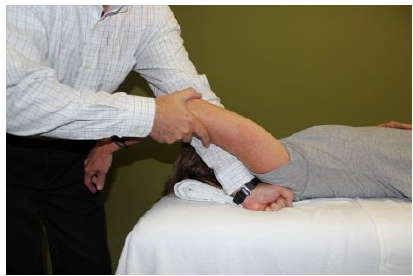
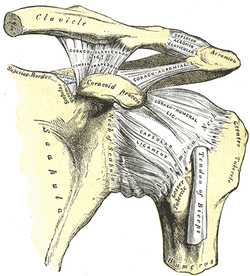 General Overview Acromioclavicular joint (ACJ) injuries are quite prevalent throughout the general population and specifically in the athletic population. In 2012 Harris et al found that ACJ disease was present in 31% of individuals who presented with shoulder pain. (Harris 2012) The ACJ is a synovial joint which connects the distal clavicle to the acromion process. The joint assists the scapulothoracic joint in full rotation to adjust for changing elevation of the humerus. Composite motion of the ACJ and sternoclavicular joint (SCJ) contributes up to 60 degrees of upward elevation, 15-30 degrees of posterior tipping, and 15-25 degrees of external rotation during arm elevation (measuring the motion at the ACJ is difficult and typically not done because the kinematics are not well defined). What we do know is that kinematics at the ACJ affect the "quality and quantity of movement at the scapulothoracic joint." (Neumann 2010) With motion occuring in 3 planes, the ACJ lacks stability and relies on 3 major ligaments for support. The acromioclavicular ligament and coracoclavicular ligaments (conoid and trapezoid) support the joint and resist horizontal stresses and limit superior translation respectively. These ligaments have fascial connections with nearby muscles, specifically the trapezius and deltoid. In a high grade AC joint separation, a clinician will often find these muscles injured as well. The resting position of the ACJ is the arm at the side and the closed packed position is full elevation. Due to the high prevalence of dysfunction, assessing the ACJ needs to be a priority during an initial evaluation with a patient who presents with shoulder pain. 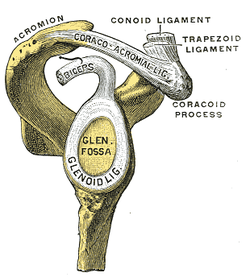 Manual Therapy Now that we know more about the ACJ, how can we treat this joint when suspecting hypomobility? Since the ACJ is a planar joint, normal concave/ convex rules of manual therapy do not apply. Therefore, we must use our clinical judgement as to when and why to perform joint mobilization or manipulation. A major factor to consider is the patient's acuity. (The novice clinician should be aware that acute ACJ separations do not require intense manual therapy because of the acuity of their symptoms and the laxity present in the region.) Generally in more acute stages, posterior to anterior ACJ mobilizations in supine with the arm resting at the side are effective (left picture below). Remember, this is the resting position of the joint as well allowing for more mobility. As the patient's ROM and strength progresses, more intense manual therapy can be performed. For example, certain patients may only have pain and limitations at end range of motion. To reach full humeral flexion and external rotation at least 30 degrees of upward rotation and 8 degrees of external rotation is needed. (Teece 2007). An example of a more advanced manual technique is a posterior to anterior mobilization at end range using the arm as a lever. In this position, the therapist's hand blocks movement of the distal clavicle so that acromion is mobilized on the stabilized clavicle. Small oscillations of the humerus are made at the end-range promoting movement at the ACJ. There are many more mobilization and manipulative techniques and positions that can be performed at the ACJ. Hopefully this post gave you an insight into a beginner and a advanced mobilization technique. -Jim
References:
Harris, Kevin D., Gail D. Deyle, Norman W. Gill, and Robert R. Howes. "Manual Physical Therapy for Injection- Confirmed Nonacute Acromioclavicular Joint Pain." Journal of Orthopaedic & Sports Physical Therapy 42.2 (2012): 66-80. Print. Neumann, Donald A. Kinesiology of the Musculoskeletal System: Foundations for Physical Rehabilitation. St. Louis: Mosby, 2002. N. pag. Print Teece, Rachael M., Jason B. Lunden, Angela S. Lloyd, Andrew P. Kaiser, Cort J. Cieminski, and Paula M. Ludewig. "Three-Dimensional Acromioclavicular Joint Motions During Elevation of the Arm." Journal of Orthopaedic & Sports Physical Therapy 38.4 (2008): 181-90. Print.
4 Comments
Katie
6/11/2017 11:46:29 am
This article is very helpful and succint! My DPT program didn't spend much time on the AC joint so this is a great resource. 3/18/2024 02:44:01 am
Manual therapy is a crucial component in alleviating AC joint pain, offering relief and promoting healing. Techniques such as mobilization and manipulation aid in restoring joint function and reducing discomfort. In cases where conservative measures prove insufficient, individuals may opt for AC repair in Kyle, TX, a surgical intervention aimed at addressing severe joint damage. However, manual therapy often serves as an initial step in managing AC joint issues, fostering improved mobility and enhancing overall well-being through targeted therapeutic approaches. 4/26/2024 04:44:32 am
I particularly found the section on specific manual therapy techniques and their application very informative. It's empowering to know that there are effective, non-invasive treatments available for AC joint pain, and your article does an excellent job of highlighting them. Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|

 RSS Feed
RSS Feed