
|
|
|
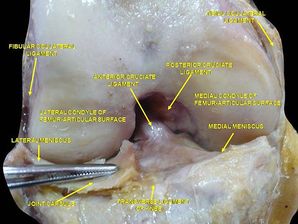
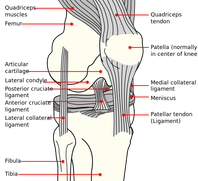
 A few weeks back I posted an article discussing a recent knee injury I sustained. In that post I outlined several important pieces of information often under-looked when rehab'ing a knee. As of last week, my rehabilitation was going great: I had returned to running for >1 hour, performing weighted squats, and only having pain at end-range flexion. This all changed 1 week ago when I returned to wake boarding for the first time. While performing a trick, I landed wrong and re-injured my knee. I experienced similar symptoms to my first injury: a pop, immediate pain, and swelling. Under the supervision of a nurse practitioner, we agreed it would be best for me to get an MRI to rule out ligament or osteochondral lesions (Phisikil 2006). The MRI impression (verbally per NP): 1) Meniscofemoral ligament rupture 2) MCL and ACL sprain (fortunately not torn) 3) Intact meniscus 4) No chondral lesions Based off the impression, it appeared I dislocated my patella during the injury (unknown to me). Once again I needed to start conservative management. In this post I am going to do a brief knee anatomy review of the ACL and MCL as well as discuss conservative management of these injuries.
Conservative management of an MCL injury: Non-operative management has been proposed as the mainstay treatment for MCL injuries (Phisikil 2006). With an isolated MCL injury, treatment consisting of protected ROM and progressive strengthening has been shown to produce excellent results. During the inflammatory phase, use the RICE principle to minimize pain and swelling. Use crutches until the individual can walk without a limp. As the patient progresses, both the stair climber and the bicycle ergometer are easy methods of maximizing ROM and minimizing stiffness. Once range of motion is restored, lower extremity progressive resistive exercises should be initiated. I have been following the above protocol closely with good success. One consideration I need to take into account is the concomitant ACL sprain. Although the research is lacking on multi-ligament conservative management, I am guiding my ACL rehab by both pain and the knowledge of ACL stress/strain. Since my ACL is healing, I want to avoid exercises that place excessive strain across the ligament. At the same time, the ligament does need some stress to allow for normal collagen realignment. Thus far I have mainly been performing closed chain activities and riding the bicycle. Fortunately I do not have any meniscal or articular cartilage damage which allows me to progress loading at a faster rate. I hope this mini-anatomy and conservative management review was helpful. -Jim References:
Phisitkul P., James S.L., Wolf B.R., Amendola A. (2006) MCL injuries of the knee: current concepts review. Iowa Orthopaedic Journal 26, 77-90
1 Comment
Christian
8/22/2014 01:51:17 am
Thanks, Jim - always helpful. Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|
 RSS Feed
RSS Feed