
|
|
|
 The overhead athlete is a unique type of athlete to treat in physical therapy. When I think about the different types of overhead athletes I include the baseball thrower, tennis player, and even the quarterback. Each of the mechanics of these athletes is different and present unique challenges (load, speed, intensity, biomechanics, etc). However, while each of these athletes are different, some of the exercises can be tailored to each sport. Recently, I was working with a competitive high school tennis player. He presented with a very stiff shoulder and diffuse pain. When I say stiff shoulder, I mean he had very limited shoulder flexion, abduction, and inability to get into a 90/90 position without pain. His postural presentation was a significantly lax R shoulder (hanging down), flat t-spine, and scapular winging. After some time working on pec minor, lat, and subscap tone he was able to start to recruit some of his scapular stabilizers (primarily serratus & low trap) much better. However, his rehabilitation took off once he had good shoulder flexion ROM and we were able to start to work on overhead stability. So what overhead stability exercises did I use?
What else do you use for overhead stability? Comment below and let me know - Dr. Brian Schwabe, PT, DPT, SCS, COMT, CSCS Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly. 
1 Comment
 Adhesive capsulitis (a.k.a frozen shoulder) is associated with synovitis and a capsular contracture of the shoulder joint. (1) Patients with frozen shoulder often have limited active and passive range of motion, significant pain throughout their shoulder range of motion, and associated upper quarter muscle strength deficits. Since the joint capsule is suggested to be the structure limiting movement, range of motion deficits are often greatest in shoulder external rotation > abduction > internal rotation. While adhesive capsulitis is often thought to be a self-limiting condition, studies have reported "ranges of between 20 and 50% of patients with adhesive capsulitis which suffer long-term ROM deficits that may last up to 10 years." (2) As a healthcare practitioner it is important to know the expected prognosis and understand the potential for long-standing symptoms does exist. It is also important to understand what is the current best evidence for treatment of adhesive capsulitis and common management strategies if conservative management fails. In this post, I will be discussing one of the surgical management options for adhesive capsulitis: Shoulder Manipulation under Anesthesia (MUA). How is a Manipulation Under Anesthesia Performed?While several different approaches exist, here is the shoulder manipulation under anesthesia technique as outlined by Shoulder Doc (see reference below): "The surgeon should stand at the head end of the table with one hand stabilizing the scapula in the resting position. The surgeon's other hand should then be placed in the patient's axilla such that the surgeon's forearm is resting against the whole of the inside of the patient's arm. First, abduction is taken to the patient's free limit, and then the patient is forcibly abducted while the scapula is maintained down in the anatomic position. The scapula must not move at any stage. This maneuver will rupture the inferior capsule. The shoulder is then forcibly adducted such that the affected elbow is pushed in front of the patient's chin to rupture the posterior capsule. Finally, forcible external rotation and internal rotation are added, but great care is taken here because it is during these final rotation maneuvers that a spiral fracture can be caused." (3) 
As a DPT, What Should I Consider Post-Manipulation?1. Post-manipulation range of motion should be initiated within the first few days following the procedure. This will vary from surgeon to surgeon, but many protocols recommend physical therapy within 24 hours post-surgery. Early range of motion and education is essential! 2. While the manipulation is targeted at the joint capsule, other structures are likely to be torn or injured. A 2005 study by Loew et al assessed 30 subjects with shoulder synovitis following MUA. They found "the capsule was seen to be ruptured superiorly in 11 patients, the anterior capsule was ruptured up to the infraglenoid pole in 24 patients, and 16 patients each had a capsular lesion located posteriorly. In 18 patients no additional joint damage was found after manipulation. In 4 patients, iatrogenic superior labrum anterior-posterior lesions were observed. Further injuries detected were 3 fresh partial tears of the subscapularis tendon, 4 anterior labral detachments (1 with a small osteochondral defect), and 2 tears of the middle glenohumeral ligament." In other words, the manipulation is not a specific technique. 3. Due to the amount of stress across the shoulder, mitigating pain while maximizing range of motion should be your primary focus of treatment!  What is my Patient's Prognosis After Manipulation?Depending on the research article, the post-manipulation prognosis is scattered with results ranging from no effect to moderately effective. Per the clinical practice guidelines on Shoulder Pain and Mobility Deficits: Adhesive Capsulitis, there is Grade C for effectiveness of a MUA. This indicates relatively weak evidence for use of the intervention in individuals who are not responding to conservative care.  Picture taken from Shoulder Pain and Mobility Deficits: Adhesive Capsulitis, page A23. My Clinical RecommendationDespite the weak evidence, we will continue to see these patient's post-surgery. When explaining the evidence and procedure to your clients, be honest and upfront regarding the procedure, but do not perseverate on the other injured anatomy or weak evidence for outcomes. This information can create a negative mental impression of conservative treatment, and reduce the overall patient outcome. Focus on treating that individual patient and reinforce positive improvements in their range of motion and strength. While our current evidence is lacking, that does not have to dictate the outcome with future patients! -Jim Heafner PT, DPT, OCS References: 1. Adhesive Capsulitis - Physiopedia, universal access to physiotherapy knowledge. Physio - pediacom . 2017. Available at: http://www.physio - pedia.com/Adhesive_Capsulitis. Accessed March 28, 2017. 2. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: a prospective clinical study with an evaluation of three treatment regimens. Ann Rheum Dis. 1984;43:353–60. doi: 10.1136/ard.43.3.353. 3. Manipulation under Anestesia. Shoulder Doc. 2017. Available at https://www.shoulderdoc.co.uk/article/1223. Accessed 12/25/17. Learn more from us at TSPT on our Insider Access Library
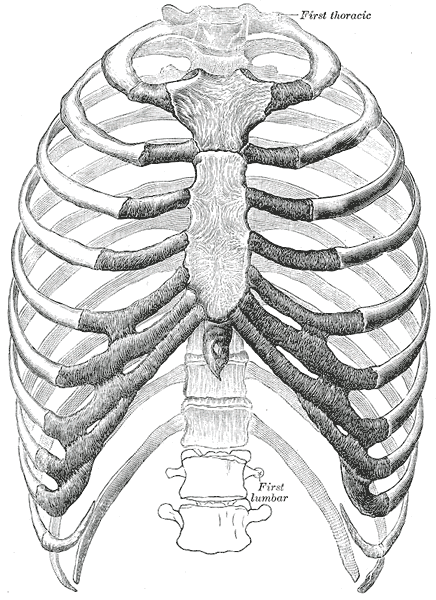
Something I have been assessing more lately is rib mobility for my upper quarter patients. In the past, unless there were signs indicative of rib dysfunction, I typically only checked the 1st rib's mobility. Lately, I have been assessing ribs 2-4 (and further down if significant restriction noted) for many of my upper quarter patients and seen some interesting effects.
Several patients I've seen recently with scapular and/or posterior shoulder pain have presented with restricted rib 2-4 mobility (or some variation). They didn't have any pain with breathing, however, had significant reduction in pain and improved mobility following simply grade IV mobilizations to the restricted ribs. Even greater improvement was noted in the following day. Now the mechanism is not fully understood as manual therapy can have quite a few different effects. It's possible the patient would have had just as effective or more effective response to other treatments. Nonetheless, with the excellent response by my patient, I plan on regularly incorporating upper rib assessment to determine if there are some patterns for application. -Dr. Chris Fox, PT, DPT, OCS Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly.   A common piece of advice for preventing overuse injuries in athletes is to cross-train. It's not wise to pitch for 12 months or only do long distance running. Sure there are outliers that can do it, but it does allow the body to recover actively. A runner may benefit from swimming or lifting weights. A basketball player may benefit from playing soccer. There are plenty of other examples for different sports and different athletes. The same concept applies to work situations and posture. There is nothing wrong with a job that requires lots of sitting or activity that requires repetitive tasks; however, again it may beneficial for a change in activity occasionally. For example, a job that requires lots of sitting may benefit from switching to standing occasionally, or going for a walk, or doing some regular stretching. I spoke with a patient recently about her son that cut firewood for a living. Apparently, he was having some arm and shoulder pain recently from working overtime. While he may benefit from some physical therapy, it may be that he just needs some general strengthening exercises. Recently, I have heard some discussion about research that shows general strengthening can be just as effective as specific exercise. While this may be true, I believe that depending on the activity of the individual, there may be more some beneficial general exercises than others. For example, an individual with shoulder pain that does repetitive work in front of them may benefit from general back/shoulder strengthening. An individual with repetitive lumbar flexion tasks may benefit from regular lumbar extension strengthening. Some may find it threatening to our ability as PT's that we no longer have to be "experts" with exercise prescription. Instead, we should focus on how this may improve our patient's potential prognosis. The less patient's feel like they NEED us to hold their hand in their recovery and the more we make them independent with managing their injury, the better our care can potentially be. Overall, the final message I want to give is that a lot of injuries may benefit from a general strengthening approach. We may not need to be as specific with our strength testing in most cases, but there may still be instances where being thorough with an evaluation will pick up some severe pathologies. I typically perform the same base evaluation for upper quarter patients and then lower quarter patients and then add in specific tests as needed. Barring any significant findings, a lot of exercises that I prescribe are similar. This may be due to common pathologies and impairments associated with them or it may be due to a response to general strengthening. -Dr. Chris Fox, PT, DPT, OCS TSPT is now offering a comprehensive LUMBAR SPINE COURSEInterested in learning more about the lumbar spine?
Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly.  Chronic pain remains one of the most difficult diagnoses to treat. Over the years, various treatment styles have come through claiming to be the "fix" for chronic pain: McKenzie, core stabilization, dry needling, manipulation, etc. The current best-evidence approach incorporates much of what pain science research has revealed recently.  One of the most important concepts for managing our patient's pain experience lies in educating them about what is pain and how the nervous system works. There are an enormous amount of factors that contribute to a individual's experience: work, family, finance, and much more. Explaining to our patients how these factors can impact them is essential. While the purpose of this article is not to teach you how to educate your patients about pain, there are plenty of resources out there. We recommend Explain Pain, Therapeutic Neuroscience Education and videos like the two shown below.
Another useful component for managing chronic pain includes graded exposure. Graded exposure involves gradually increasing the tolerance to certain activities that patients are afraid will "hurt." There's a lot more to it than that, but we recommend finding an activity or function that the patient is currently having a difficult time doing, but is one of the primary goals. We want to make it so the patient is even more motivated to work towards it. Next, you find different ways to gradually increase the exposure to those activities and increase the "tolerance." For example, if your patient is having a hard time walking and that is their goal. You may challenge them to simply focus on gradually increasing their walking distance each week. Don't tell them to focus on how much pain they are experiencing. Reinforce the goal of improving their function. Another method may be to alter the actual load gradually. Walking in a pool or on a body weight supported treadmill can be useful in increasing walking and aerobic activity, while not letting the patient's pain limit them. Over time, the body weight % can be increased, so that eventually they are walking further on land. There are many ways to address low back pain and each individual may respond differently, but patients with chronic pain can be a little more difficult to manage. Consider incorporating pain science education and graded exposure to your treatments. These patients do not typically have the same "mechanical" response as more acute cases. -Dr. Chris Fox, PT, DPT, OCS TSPT is now offering a comprehensive LUMBAR SPINE COURSEInterested in learning more about the lumbar spine?
Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly.  "Hinge points and movement deviations may not be pertinent to pain, but they tell a story about how someone chooses to load their joints and program their movements." |

 |  | 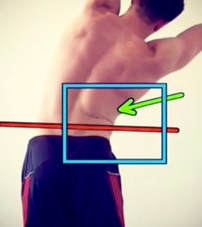 |
Picture Analysis
*Do not worry pain scientists, I know we naturally flex through the lumbar spine and some people naturally lean more forward depending on their tibia to femur ratio.
**Do not worry global strengthening folks, I know there is no evidence to support TrA activation.
***I won't get into the topic of inhibited vs. facilitated muscle groups in this post.
- Hinge point in R low back at L2 region with side bending
- Excessive lumbar flexion with forward trunk positioning during the squat
- Hinge point at L2 region during lat pull down
*Do not worry pain scientists, I know we naturally flex through the lumbar spine and some people naturally lean more forward depending on their tibia to femur ratio.
**Do not worry global strengthening folks, I know there is no evidence to support TrA activation.
***I won't get into the topic of inhibited vs. facilitated muscle groups in this post.
Pain Science Perspective
I am aware that hinge points and movement deviations on a squat are not a cause of pain. As I wrote in a blog post earlier this year, "The research does not support either good or bad posture. We cannot confidently say that poor posture causes problems OR good posture prevents problems. This is because posture alone does not equal pain. Several studies have been published over the past few years that confirm pain is unrelated to our anatomical tissues. For example, 34% of asymptomatic people >60 years old have been found to have rotator cuff tears. One in three people WITHOUT SHOULDER PAIN have a rotator cuff tear. "
However, I simply could not do enough self-neuroscience education to decrease the pain (maybe I didn't believe myself...who knows.) Despite offloading and gradually reintroducing weight to the movements, my brain continued to recognize the movements as painful.
However, I simply could not do enough self-neuroscience education to decrease the pain (maybe I didn't believe myself...who knows.) Despite offloading and gradually reintroducing weight to the movements, my brain continued to recognize the movements as painful.
At this point, I hit a crossroad. Do I...
1) Continually load the painful patterns to desensitize the movements
- This would follow the pain science path of treatment
- This would follow the movement and posture path of treatment
Self Treatment
Personally, I chose to perform a combination of both options.
My top 3 interventions:
My top 3 interventions:
- Lumbar extensions
- Hip external rotation mobility
- Thoracic mobility.
 |  |  |
1) Lumbar extensions were performed to improve lumbar extension range of motion as well as improve the loading pattern into extension as I squatted. While the first few repetitions were painful, the repeated loading desensitized movement and allowed me to maintain an upright position in the squat.
2) Hip External Rotation mobility was performed to improve the joint mobility in my hips. I perceived that tight hip joints were limiting my capacity to squat. From a mechanical standpoint, improved hip mobility allowed me to disassociate lumbar motion from pelvic motion. The increased hip mobility allowed me to maintain a neutral spine position and load through the posterior chain.
3) Thoracic mobility was performed to help maintain an upright posture during squatting movements and allow for improved shoulder mobility while performing lat pull downs. Additionally, improved thoracic mobility gave me a sense of better scapular muscle activation.
2) Hip External Rotation mobility was performed to improve the joint mobility in my hips. I perceived that tight hip joints were limiting my capacity to squat. From a mechanical standpoint, improved hip mobility allowed me to disassociate lumbar motion from pelvic motion. The increased hip mobility allowed me to maintain a neutral spine position and load through the posterior chain.
3) Thoracic mobility was performed to help maintain an upright posture during squatting movements and allow for improved shoulder mobility while performing lat pull downs. Additionally, improved thoracic mobility gave me a sense of better scapular muscle activation.
Incorporating Movement & Pain Science
In my situation, combining my knowledge of pain and tissue damage with the more mechanical approach of proper alignment was very effective. Since the brain is the control center of all input and output, it recognizes when someone is using too much energy to perform a task. For example, the forward head posture is not inherently painful, but chronic forward head positioning is an inefficient use of energy. To hold the head in a forward position, the anterior and posterior muscles are not working in equilibrium. The brain must expend more energy, time, and attention to keeping the head in a forward position. It has nothing to do with pain, and everything to do with efficiency. The combination of approaches was beneficial because I brought awareness and perception to areas that needed stimulation, and simultaneously calmed down areas that were already too sensitive to movement.
In conclusion: the treatment approach will be different for everyone. We all think, move, and act in unique ways. Many of our daily actions are performed reflexively without thought or awareness. Bringing increased perception to a painful region while modulating their pain will allow someone to understand why the pain is occurring and how to control symptoms.
In conclusion: the treatment approach will be different for everyone. We all think, move, and act in unique ways. Many of our daily actions are performed reflexively without thought or awareness. Bringing increased perception to a painful region while modulating their pain will allow someone to understand why the pain is occurring and how to control symptoms.
-Jim Heafner PT, DPT, OCS

Core strengthening appears to be a very abstract term in the world of physical therapy. To some, it means very specific motor control training. To others, it means planks. Several years ago, a proposed core stabilization clinical prediction rule was shown to lack validity. Regardless, due to the lack of established guidelines for core stability training, there will continue to be a variety of techniques, based on the clinician's preference.
When it comes to lumbar manipulation, there has been a significant amount of research to show our inability to manipulation a specific segment. Even when we try to "isolate" an area, movement can occur several segments above and below. It would appear the lack of specificity with manipulation is rather insignificant, so certain patients may just respond to manipulation in general. Can the same theory apply to stabilization? I recently read a study that compared specific motor control training in the lumbar spine to high-load deadlift training. The results showed that there was no difference in strength, pain intensity or muscle endurance between the two groups. The motor control group did have better motor control and activity, but the fact that pain, strength, and endurance were similar can help us in not needing to be so specific with our exercises. Sometimes, the particular instructions we give to our patients can actually cause a fear of movement, which is something we want to avoid.
When it comes to lumbar manipulation, there has been a significant amount of research to show our inability to manipulation a specific segment. Even when we try to "isolate" an area, movement can occur several segments above and below. It would appear the lack of specificity with manipulation is rather insignificant, so certain patients may just respond to manipulation in general. Can the same theory apply to stabilization? I recently read a study that compared specific motor control training in the lumbar spine to high-load deadlift training. The results showed that there was no difference in strength, pain intensity or muscle endurance between the two groups. The motor control group did have better motor control and activity, but the fact that pain, strength, and endurance were similar can help us in not needing to be so specific with our exercises. Sometimes, the particular instructions we give to our patients can actually cause a fear of movement, which is something we want to avoid.
Now, I am not necessarily saying there is no point to motor control training. I would simply argue that it's not as important as we used to think. If there is a subtle pelvic motion when reaching overhead, we don't necessarily need to be stopping the exercise altogether. It may still be beneficial to establish some general patterns of motion during earlier stages of rehab in order to prevent re-aggravation during high load training. Personally, following my manual treatment (if indicated), I will start with a couple mobility exercises to help get the spine moving. I then follow that up with some motor control training to prep for whatever movement I am going to have the patient perform. For example, if my patient will be doing a deadlift, I will prime them with a quad rock back and/or hip hinge, in order to help dissociate lumbar and hip motion with heavy lifting. My end-goal however, is to get my patient strengthening with heavier weight.
-Dr. Chris Fox, PT, DPT, OCS
-Dr. Chris Fox, PT, DPT, OCS
TSPT is now offering a comprehensive LUMBAR SPINE COURSE
Interested in learning more about the lumbar spine?
 | This online course includes:
|
Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly.
Cervical stability testing is one of the most important aspects of a cervical screen. While it may not help our treatment directly, it may save some people's lives or prevent significant worsening of injury. There are several key components of cervical stability testing:
-Transverse Ligament
-Alar Ligament
-Fracture Screening
There is specific testing for Alar Ligament Integrity but for cervical fx screening, it is recommended to utilize the Canadian C-spine rules and Jefferson Fx test.
The Transverse Ligament is responsible for maintaining stability between C1 and the odontoid process of C2. Without the ligament functioning, spinal cord injury is possible. While it is rare for a patient with a ruptured Transverse Ligament to present to you in a clinic, with direct access, it is certainly possible. The patient may hold their head in a certain position (avoiding positions that aggravate symptoms), to keep the injury "reduced." There are two methods that we recommend for testing the ligament's integrity: Sharp-Purser Test and Supine Transverse Ligament Test.
-Transverse Ligament
-Alar Ligament
-Fracture Screening
There is specific testing for Alar Ligament Integrity but for cervical fx screening, it is recommended to utilize the Canadian C-spine rules and Jefferson Fx test.
The Transverse Ligament is responsible for maintaining stability between C1 and the odontoid process of C2. Without the ligament functioning, spinal cord injury is possible. While it is rare for a patient with a ruptured Transverse Ligament to present to you in a clinic, with direct access, it is certainly possible. The patient may hold their head in a certain position (avoiding positions that aggravate symptoms), to keep the injury "reduced." There are two methods that we recommend for testing the ligament's integrity: Sharp-Purser Test and Supine Transverse Ligament Test.
| | |
While both tests can be effective for assessing stability, we recommend using both. First, the Sharp-Purser Test should be used as it is a REDUCING test. That means, if a symptomatic patient presents, you will reduce their symptoms if the test is positive. While most patients won't allow you to "provoke" their symptoms with the initial part of the test, it is still important to try reducing symptoms before aggravating. Next, we recommend using the supine Transverse Ligament Test to provoke symptoms. The force is minimal, so it is unlikely to be harmful if stopped when any appropriate symptoms are produced.
While the diagnostic accuracy for upper cervical stability and utilization of Canadian C-Spine rules is relatively high, it is not recommended to completely override clinical decision making. As always, we recommend a thorough evaluation and consideration of the evidence of each test's findings. For more information on these tests, be sure to check out the pages linked above.
-Dr. Chris Fox, PT, DPT, OCS
While the diagnostic accuracy for upper cervical stability and utilization of Canadian C-Spine rules is relatively high, it is not recommended to completely override clinical decision making. As always, we recommend a thorough evaluation and consideration of the evidence of each test's findings. For more information on these tests, be sure to check out the pages linked above.
-Dr. Chris Fox, PT, DPT, OCS
TSPT now offering a comprehensive Cervical Spine Course
Interested in learning more about the cervical spine?
 (Save $10 with Promo: Neckpain) | This online course includes:
|
Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly.
In honor of National Physical Therapy month, The Student Physical Therapist has compiled a list of facts, statistics, and fun information about our amazing profession. This quiz covers everything from historical facts about Physical Therapy to Physical Therapists perception on the dating app Tender!
 |  |
 |  |
Take our Quiz!
We hope you enjoy the quiz! Please continue to strive everyday to make the profession great.
#getPT1st
Jim, Chris, and Brian
#getPT1st
Jim, Chris, and Brian
Join the Insider Access Community!
 | Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added regularly. |
With the progression of evidence-based practice, much of the research that is being performed is looking to determine what treatment techniques are most effective for a variety of injuries. Included in that research is the development of clinical prediction rules (CPR's), which are used to take various exam findings and cluster them to determine more effective treatment measures. The below findings for individuals with neck pain were initially found to have significant benefit from thoracic manipulations (Cleland et al, 2007):
| -Symptoms < 30 days -No symptoms distal to the shoulders -Looking up does not aggravate symptoms -FABQ Physical Activity Scale < 12 -Diminished upper thoracic kyphosis -Cervical extension ROM < 30 deg -3 positive = +LR of 5.5 -4 positive = +LR of 12 -5-6 positive = +LR of > 12 |  |
There is an extensive process for developing a CPR that has true utilization and application. After a CPR has been proposed, it must go through a validation procedure. When reviewed, this CPR was unable to be validated (Cleland et al, 2010); however, those in the manipulation group were still found to have improved short- and long-term disability. Just because it didn't have the other original intended effects, doesn't mean it may not have a use.
Whether thinking about the thoracic spine in an anatomical sense or a neurophysiological one, manipulating the region can be incredibly useful. The T6-7 area has been shown to be a tension point as the vertebral canal is relatively narrow compared to the spinal cord here. Additionally, there is little movement in the spinal core here relative to the adjacent structures. These restrictions can affect nerve irritability and function. With manipulation and mobilization, the biomechanical aspect of nerve mobility can theoretically improve or it may simply be stimulating the nervous system in a novel way (or it may be purely psychological). Either way, manipulating the thoracic spine can be beneficial for many injuries. It's definitely a skill worth practicing and implementing!
-Dr. Chris Fox, PT, DPT, OCS
Whether thinking about the thoracic spine in an anatomical sense or a neurophysiological one, manipulating the region can be incredibly useful. The T6-7 area has been shown to be a tension point as the vertebral canal is relatively narrow compared to the spinal cord here. Additionally, there is little movement in the spinal core here relative to the adjacent structures. These restrictions can affect nerve irritability and function. With manipulation and mobilization, the biomechanical aspect of nerve mobility can theoretically improve or it may simply be stimulating the nervous system in a novel way (or it may be purely psychological). Either way, manipulating the thoracic spine can be beneficial for many injuries. It's definitely a skill worth practicing and implementing!
-Dr. Chris Fox, PT, DPT, OCS
References:
Cleland JA, Childs JD, Fritz JM, Whitman JM, Eberhart SL. "Development of a clinical prediction rule for guiding treatment of a subgroup of patients with neck pain: use of thoracic spine manipulation, exercise, and patient education." Phys Ther. 2007 Jan. Web. 08/18/2012.
Cleland JA, Mintken PE, Carpenter K, Fritz JM, Glynn P, Whitman J, Childs JD. Examination of a clinical prediction rule to identify patients with neck pain likely to benefit from thoracic spine thrust manipulation and a general cervical range of motion exercise: multi-center randomized clinical trial.
Phys Ther. 2010 Sep;90(9):1239-50.
Cleland JA, Childs JD, Fritz JM, Whitman JM, Eberhart SL. "Development of a clinical prediction rule for guiding treatment of a subgroup of patients with neck pain: use of thoracic spine manipulation, exercise, and patient education." Phys Ther. 2007 Jan. Web. 08/18/2012.
Cleland JA, Mintken PE, Carpenter K, Fritz JM, Glynn P, Whitman J, Childs JD. Examination of a clinical prediction rule to identify patients with neck pain likely to benefit from thoracic spine thrust manipulation and a general cervical range of motion exercise: multi-center randomized clinical trial.
Phys Ther. 2010 Sep;90(9):1239-50.
TSPT now offering a comprehensive Cervical Spine Course
Interested in learning more about the cervical spine?
 (Save $10 with Promo: Neckpain) | This online course includes:
|
Looking for advanced sports and orthopedic content? Take a look at our BRAND NEW Insider Access pages! New video and lecture content added monthly.

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages
Insider Access pages


We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!
Archives
July 2019
June 2019
May 2019
March 2019
February 2019
January 2019
December 2018
November 2018
October 2018
September 2018
August 2018
July 2018
June 2018
May 2018
April 2018
March 2018
February 2018
January 2018
December 2017
November 2017
October 2017
September 2017
August 2017
July 2017
June 2017
May 2017
April 2017
March 2017
February 2017
January 2017
December 2016
November 2016
October 2016
September 2016
August 2016
July 2016
June 2016
May 2016
April 2016
March 2016
February 2016
January 2016
December 2015
November 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
February 2015
January 2015
December 2014
November 2014
October 2014
September 2014
August 2014
July 2014
June 2014
May 2014
April 2014
March 2014
February 2014
January 2014
December 2013
November 2013
October 2013
September 2013
August 2013
July 2013
June 2013
May 2013
April 2013
March 2013
February 2013
January 2013
December 2012
November 2012
October 2012
September 2012
August 2012
Categories
All
Chest
Core Muscle
Elbow
Foot
Foot And Ankle
Hip
Knee
Manual Therapy
Modalities
Motivation
Neck
Neural Tension
Other
Research
Research Article
Shoulder
Sij
Spine
Sports
Therapeutic Exercise
 RSS Feed
RSS Feed