
|
|
|
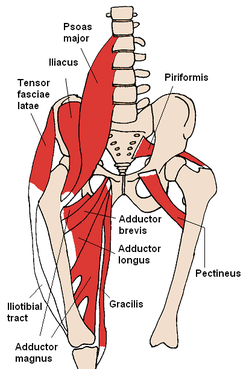 Last week, I evaluated a patient with neck and back pain s/p MVA. The patient presentation was pretty typical in regards to whiplash as far as aggravating and alleviating factors go. One thing that did stand out, however, was the presence of knee pain. The patient denied any trauma to the knee during the accident and has noticed it being far worse in sitting. This can lead one to a couple hypotheses, such as the presence of swelling with the knee in the 90 deg flexed position or neural tension causing the pain. Due to the lack of trauma and the patient not being able to pin point any one spot for the knee pain (medial knee pain into proximal medial tibia), I was leaning towards saphenous neural tension. As with any other hypothesis, additional testing is required to either increase or decrease likelihood. During my objective evaluation, I found several objective measures that increased my suspicion of a neural component at the knee: dysfunctional and painful lumbar extension and restricted lumbar sideglides to the involved side, positive slump test for reproduction of knee pain, no significant in findings of examination of the knee. Another finding that stood out to me was a reproduction of his knee pain with resisted hip flexion (not with palpation of the knee). This sort of finding brings to mind potential hip diagnoses such as SCFE, Legg-Calve-Perthes, Hip OA, etc., but the patient at arpproximately 40 years old didn't fall into the typical demographic for these pathologies. An additional explanation can be due to contraction of the Iliopsoas muscle. Remember the anatomy of the muscle: -Origin: (Psoas Major portion) ventral surfaces of the transverse processes of all lumbar vertebrae, sides of the bodies and corresponding intervertebral disks of the last thoracic and all lumbar vertebrae, and the membranous arches that extend over the sides of the bodies of the lumbar vertebrae; (Iliacus portion) superior 2/3 of the iliac fossa, internal lip of the iliac crest, iliolumbar and ventral sacroiliac ligaments, and ala of the sacrum. -Insertion: Lesser trochanter of the femur. The big thing to take away from the musculature attachments is the axial compression force that occurs with contraction. By compressing the spine, when the lumbar spine is irritated, neural symptoms can be produced, which is why the patient's pain was reproduced with neural tensioning. While the patient may benefit from some local treatment to the knee to decrease the neural symptoms, the primary focus of treatment must be on the back. Due to time constraints, I was unable to trial repeated motions, but that likely will be a significant part of my plan of care for both the neck and back pain, which may reduce the knee symptoms as well. -Chris References:
Kendall FP, McCreary EK, Provance PG, Rodgers MM & Romani WA. Muscles Testing and Function with Posture and Pain, 5th ed. Baltimore, MD: Lippincott Williams & Watkins. 2005. 422-423. Print.
1 Comment
chad
1/21/2015 11:29:43 pm
Interesting case, it seems that this patient's problem is indeed from the lumbar spine based on your description. Your explanation of the compressive effects of the iliopsoas on the spine is something I have never thought about as a way to incorporate into eval of a patient presenting as this one does. Great example of using anatomy to "think outside of the box" Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|
 RSS Feed
RSS Feed