
|
|
|
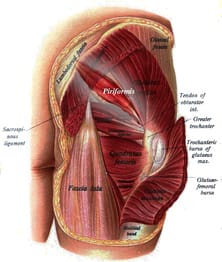 One of the frustrating aspects of research studies that is often overlooked is that patient population, and, more specifically, the diagnostic criteria for that population. Without a specific diagnosis (and conclusive method of diagnosing), the study immeidately presents with multiple confounding variables. Our ability to assess the benefit of an experimental intervention becomes inconclusive when there is a lack of homogeneity in the group. In one of mentoring sessions at Optim, there was a disagreement about pain referral patterns for piriformis syndrome. One individual stated that research well-supported piriformis syndrome up to the spine. I had disagreed as typically pain does not refer that far upwards. Of course, after hearing this disagreement, I went ahead to looked at some of the research behind piriformis syndrome. In this systematic review, the article basically starts out with explaining on piriformis syndrome is a controversial diagnosis and we have little to no clinical ability to diagnose it. Moving onto the actualy results, there was between 14-63% participants with low back pain. Looking simply at the results, it would appear that low back pain is a common finding in those with piriformis syndrome. However, based on the fact that we have difficulty even diagnosing the pathology, we can't rule out the possibility (in my opinion, likelihood) that the lumbar spine may be the source or the primary component (think Double Crush Syndrome). This conflict should basically have stopped the study as all findings, in reality, have fault in basis. So what does this mean clinically? For me, not much. I treat the impairments primarily in my patients. If a patient did come in with "piriformis syndrome," I'm going to address any lumbar mobility restrictions I find. If the hip is weak, I'm going to strengthen it. That be said, there are some conditions where specific diagnoses do have clinical impact. For example, if a specific diagnosis has been shown to benefit significantly from a particular intervention, that will absolutely be included. In most cases, we need to be more critical analyzing all aspects of the article, especially the population/diagnostic criteria before we implement the results in our practice. Evidence-informed, not evidence-restricted. -Dr. Chris Fox, PT, DPT, OCS Reference: Kevork Hopayian,1,3 Fujian Song,1 Ricardo Riera,2 and Sidha Sambandan1. The clinical features of the piriformis syndrome: a systematic review. Eur Spine J. 2010 Dec; 19(12): 2095–2109.

2 Comments
Mary Kate Mcdonnell
1/2/2017 07:10:05 am
Agree with post. Better to make distincton of Diagnosis as a Medical Diagnosis. Agree. Medical dx may not be well defined and does not always direct a PT. Consider, using movement system dxs along with medical dx to direct PT intervention. Ex- piriformis syndrome = PT dx - Hip Addiction Medial Rotation Syndrome. (Sahrman, SA. Movement System Dx. Mosby) Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|

 RSS Feed
RSS Feed