
|
|
|
|
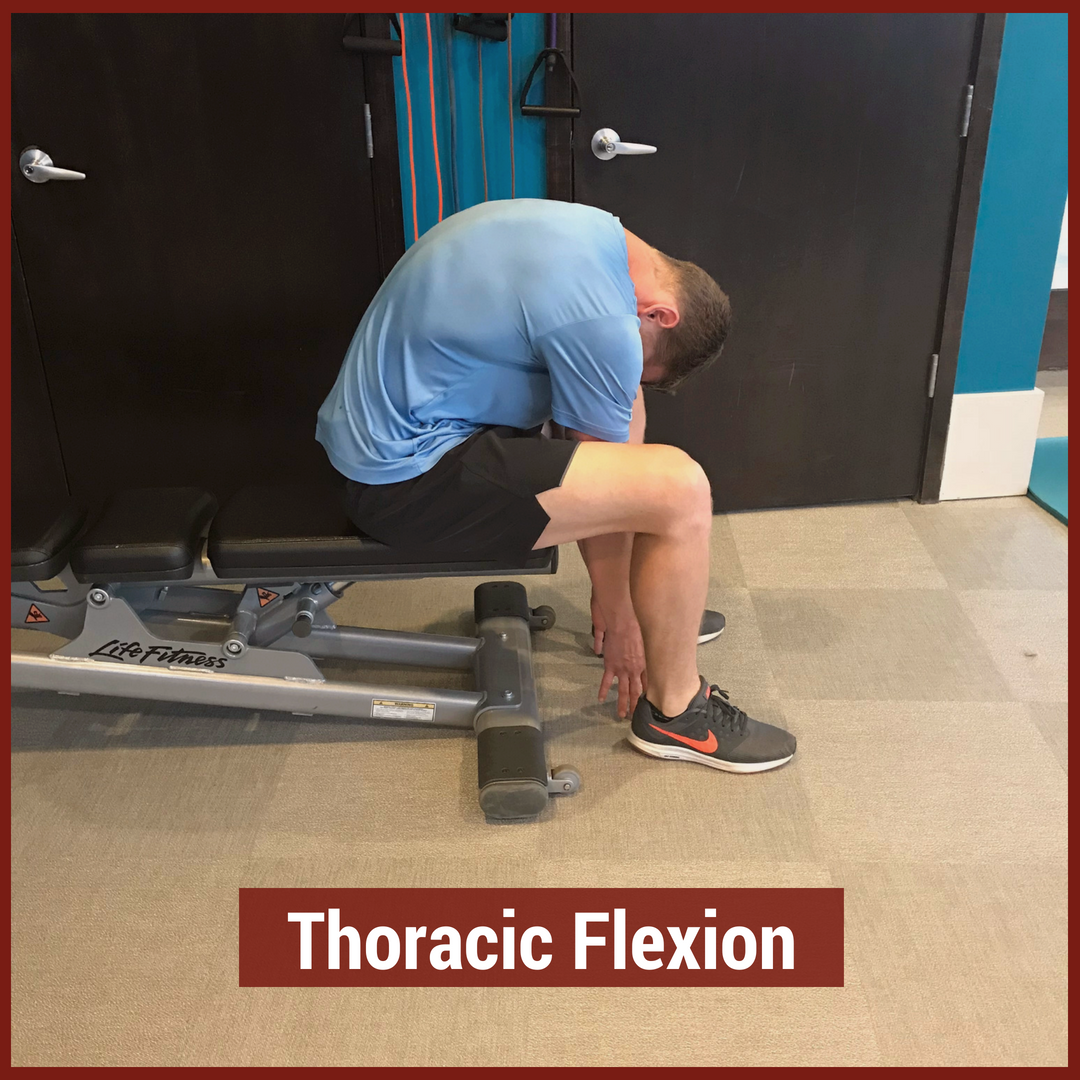
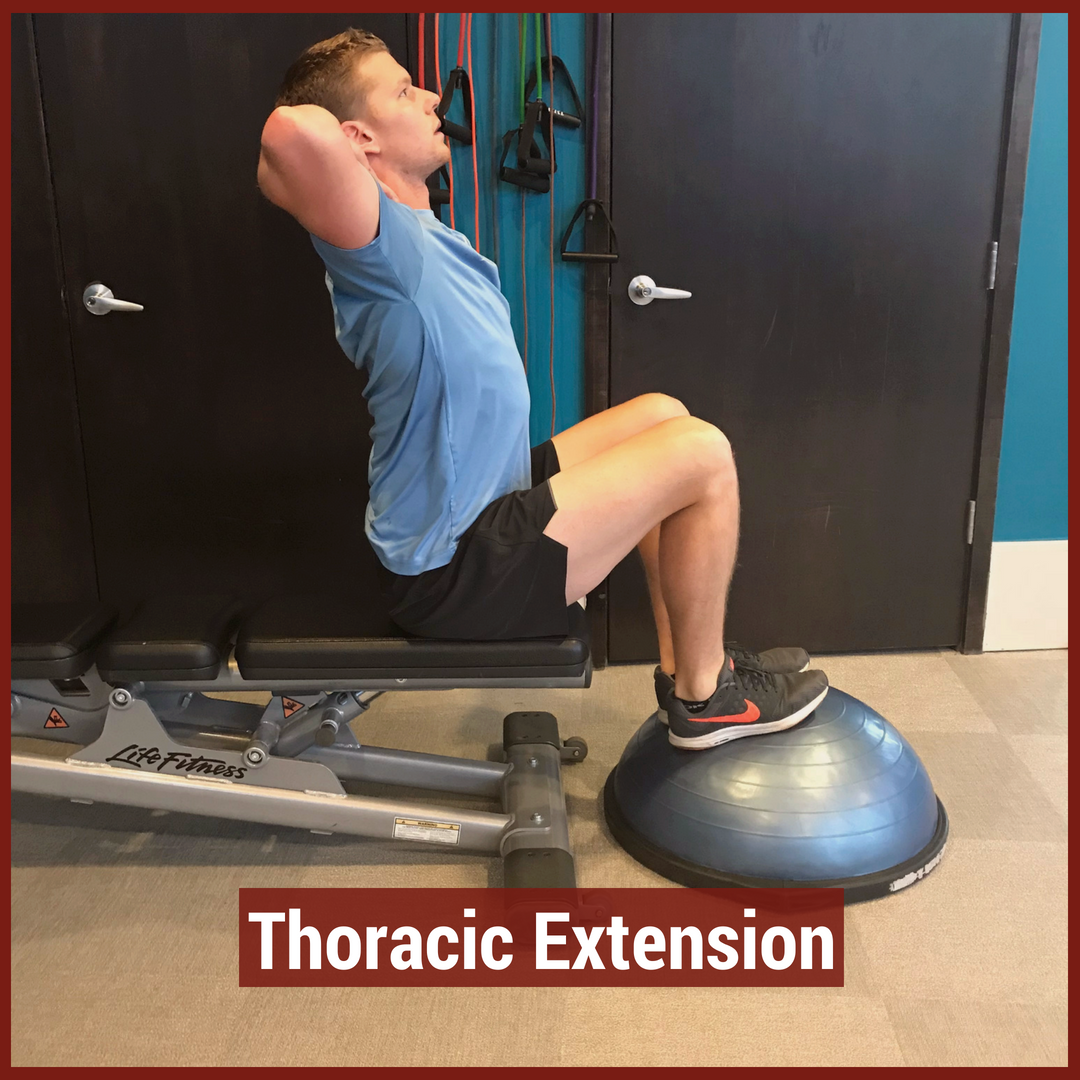
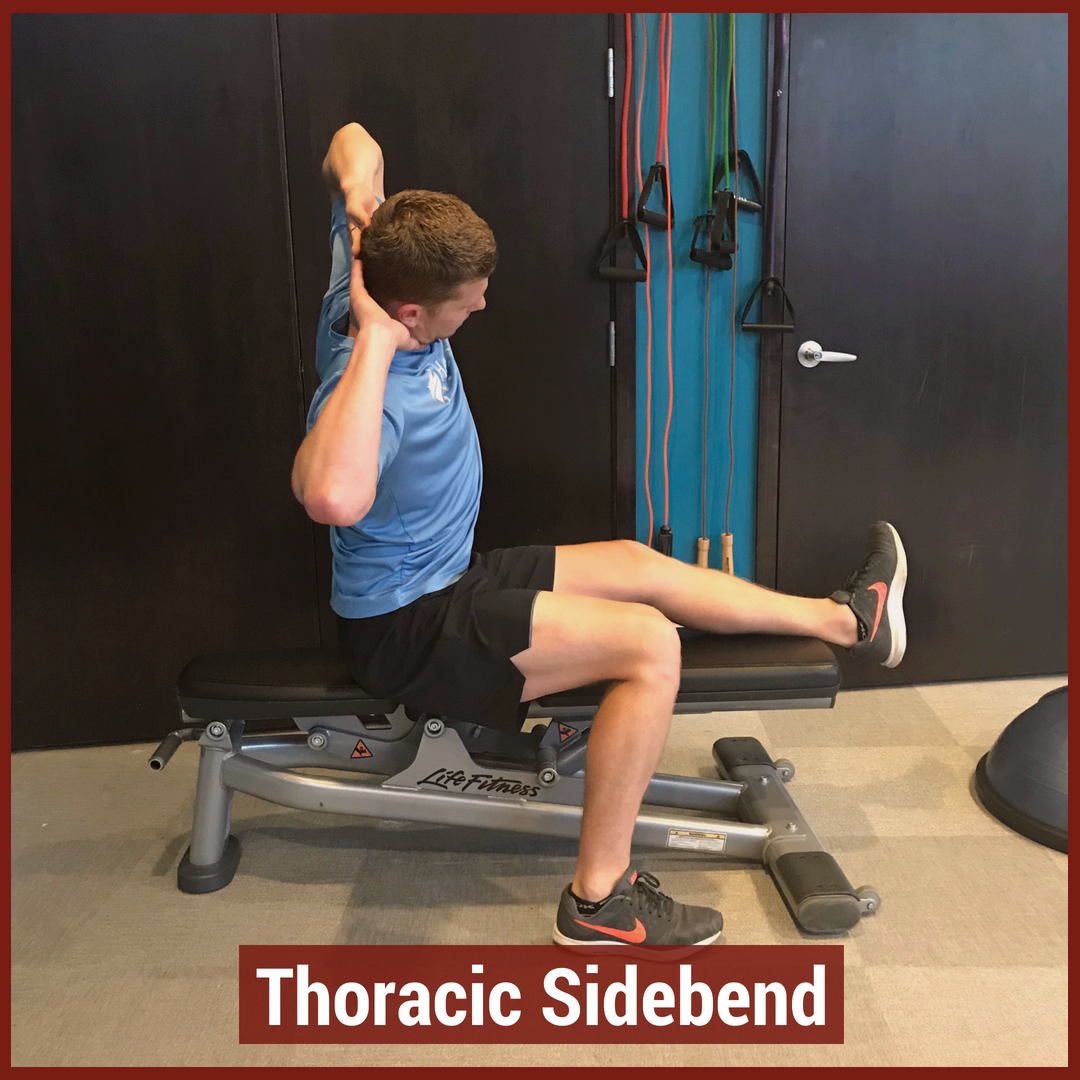
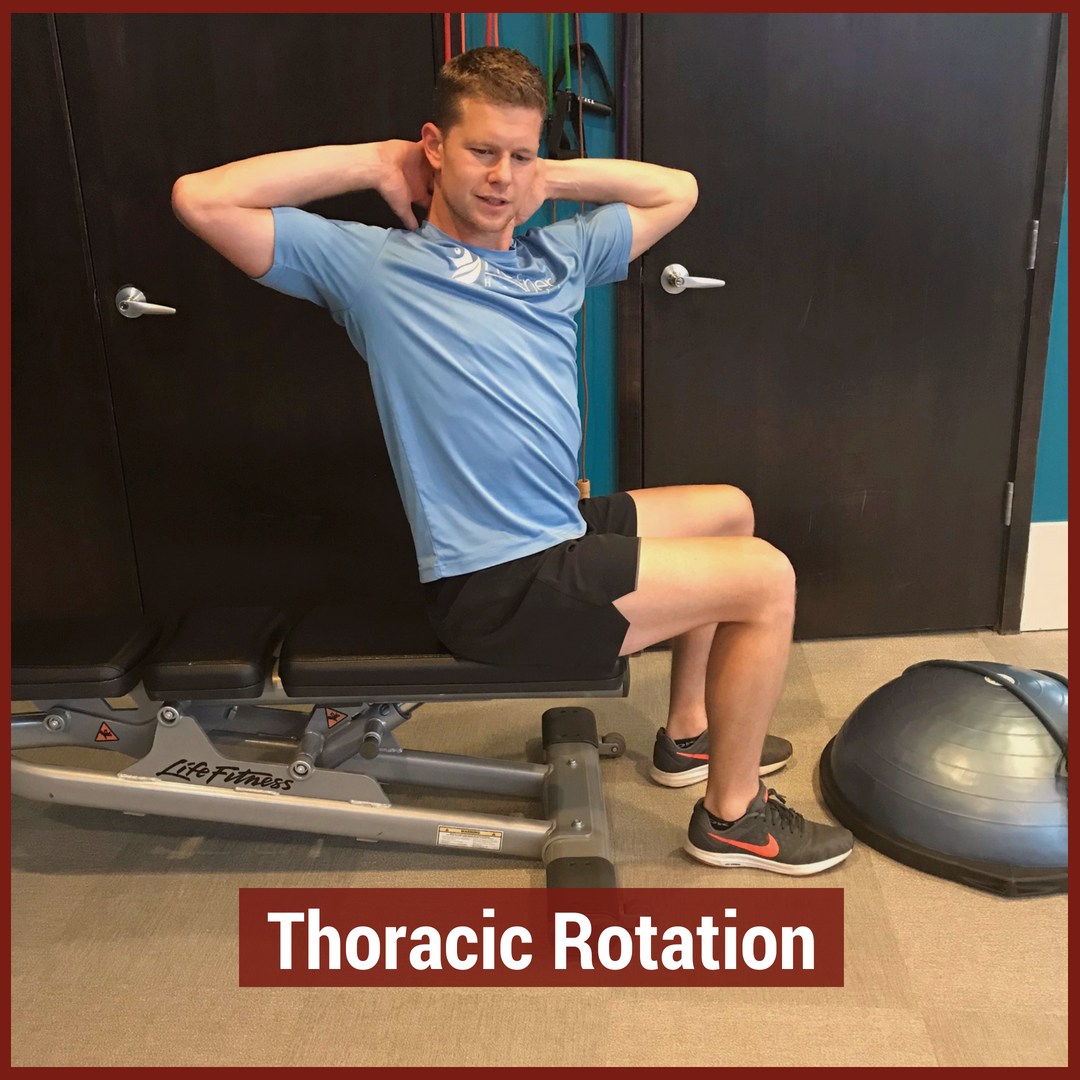
In physical therapy school, the thoracic spine is often glossed over during the musculoskeletal courses. This may be due to the low incidence and prevalence of thoracic spine pain. The incidence of thoracic spine pain is only ~15-19% across the population. This is relatively low compared to lumbar spine pain, which has an 80% prevalence in adults. Additionally, physical therapy schools may choose to emphasize the non-musculoskeletal diagnosis that are important in the thoracic spine. Since many organs are housed in the thoracic cavity, hours are spent on non-musculoskeletal diagnosis. For example, if a patient presents with thoracic spine pain, it is more important to rule-out a myocardial infarction than a thoracic facet restriction. Regardless, there is a gap in student's knowledge regarding thoracic spine anatomy and biomechanics, mobility assessment, and differential diagnosis. In this post, I will be reviewing the active range of motion and segmental mobility assessments for the thoracic spine. Additionally, I have added some clinical pearls for thoracic anatomy and biomechanics! Anatomy and Biomechanics Review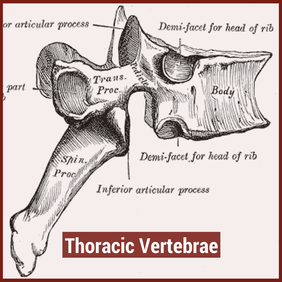 The thoracic spine is comprised of 12 vertebrae. These vertebrae have similar characteristics to cervical and lumbar spine- a vertebral body, pedicles directed posterior from the body, lamina that connect to form a spinous process, vertebral facets, and costal demi-facets (Neumann, 2010). The superior and inferior facets of the vertebrae are oriented ~60 degrees from the horizontal plane and ~20 degrees from the frontal plane. Since the thoracic spine connects cervical to lumbar, the junctional regions are important considerations as well. When transitioning from one region, there is no immediate change between cervical to thoracic vertebrae and thoracic to lumbar vertebrae. The superior thoracic vertebrae bare qualities similar to the cervical spine and the inferior thoracic vertebrae resemble the lumbar spine. This may explain why stiffness is often noted in these regions. 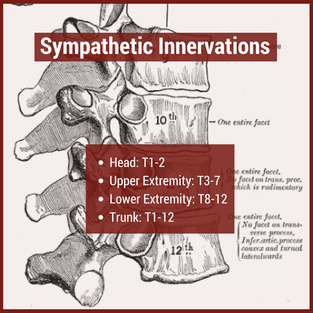 Additionally, the thoracic spine houses the sympathetic nervous system. The sympathetic nerve trunk lies anterior to the costotransverse joints. Clinically, this may help explain unusual symptoms that can be reproduced by neural tension tests such as the SLUMP TEST or Straight Leg Raise Test. Sympathetic innervations of the head arises from T1-T2, the upper extremities from T3-T7, the lower extremities from T8-T12 and the trunk from T1-T12. As Dr. Chris Fox wrote in a previous post on thoracic spine anatomy, "In the thoracic spine, T4-9 is known as the critical zone because the vertebral canal is narrowest here; it also has reduced blood supply (Egan et al, 2011). T6 is a tension point; here motion of the spinal core versus canal converge in different directions." Improving the neural mobility in the thoracic spine can help improve movement and decrease pain in the joints above and below. Active Motion AssessmentBelow are descriptions and pictures of thoracic spine active range of motion assessment. While it is impossible to isolate the thoracic spine, certain pelvis and lumbar spine positions can give the therapist a better idea of thoracic motion. In addition to the pictures below, I also assess thoracic flexion, extension, and rotation range of motion in quadruped.
Segmental Mobility AssessmentSegmental mobility is used to determine how much motion is available at each segment. In theory, this assessment is more specific than an active range of motion assessment as it tries to isolate each segment of the spine. While segmental mobility has been shown to have weak inter-rater reliability, practicing the assessment technique can be useful for improving tissue palpation and improving one's hands-on skills. Additionally, this assessment can help guide interventions when clustered with a patient's other symptoms.
Citations:
1. Briggs AM, Smith AJ, Straker LM, Bragge P. Thoracic spine pain in the general population: Prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskeletal Disorders. 2009;10:77. doi:10.1186/1471-2474-10-77. 2. Ganesan S, Acharya AS, Chauhan R, Acharya S. Prevalence and Risk Factors for Low Back Pain in 1,355 Young Adults: A Cross-Sectional Study. Asian Spine Journal. 2017;11(4):610-617. doi:10.4184/asj.2017.11.4.610. 3. Neumann, Donald. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation. 2nd edition. St. Louis, MO: Mosby Elsevier, 2010. 322-323. Print. 4. Egan W, Burns S, Flynn T, and Ojha H. The Thoracic Spine and Rib Cage: Physical Therapy Patient Management Utilizing Current Evidence. Current Concepts of Orthopaedic Physical Therapy, 3rd Ed. La Crosse, WI. 2011.
0 Comments
Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|
 RSS Feed
RSS Feed