
|
|
|
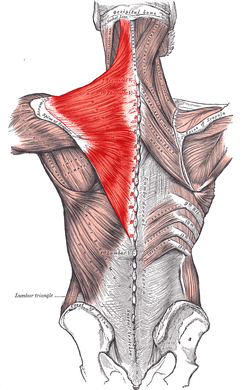
With the common perception that the UT is often short (especially with patient reports of the muscle feeling "tight" when put on stretch - of course), it is not surprising that stretching is frequently prescribed for the muscle in patients with neck and/or shoulder pain. That's not to say it is never warranted. If the muscle length is truly assessed and found to be adaptively shortened (and non-painful), of course we want to stretch the muscle. However, we must be certain that the muscle is indeed shortened first. If the UT is truly shortened, you will find the entire shoulder heightened compared to normal, meaning both the superior angle and acromion of the scapula. Often patients are seen with an elevated superior angle but depressed acromion, suggesting a downwardly rotated scapula - components of an overactive/shortened levator scapula. An exercise commonly performed at the gym involved shoulder shrugs holding weights with the idea that the individual is strengthening the UT. However, in this position, the scapula is rotated downward and results in strengthening/reinforcing the levator scapula muscle (Sahrmann, 2002). An overactive UT is also frequently accused as the culprit in shoulder impingement. However, remember that about 1/3 of shoulder elevation is due to upward rotation of the scapula, an action of the UT. Frequently, the patient will display elevation of the scapula when trying to flex or abduct the humerus. Attention should be paid to whether or not the scapula is in upward or downward rotation with that elevation. If it appears to be downward rotation, it is essential that the UT undergoes retraining. In order to focus on the UT, the shoulders should be placed in at least 90 degrees of elevation in order to place the scapula in upward rotation and allow the shrugging aspect of the motion to come from the UT, not just the levator scapula. An additional point that should be considered is the impact on the cervical spine. Sahrmann places a strong emphasis on relative stiffness and hypermobility vs. hypomobility in her teachings. As previously discussed, the UT attaches to the cervical spine and, in doing so, can be responsible for pain at the attachment site. There are at least two possible reasons for cervical pain resulting from UT impairment. One, the UT is overactive and stronger compared to the cervical intrinsic muscles. When the muscle contracts such as during upper extremity elevation, cervical extension or rotation is frequently seen (Sahrmann, 2002). You can even feel the individual cervical vertebrae rotating during shoulder flexion/abduction. This hypermobility (a precursor to hypomobility) provides the excess stress that can lead to degeneration and, in the long run, hypomobility. In this case, the UT needs to be retrained with an emphasis placed on maintaining cervical stability and neutral cervical positioning. Two, the UT is insufficient and lengthened, resulting in a pull on the proximal attachment (cervical vertebrae) due to the weight of the scapula and upper extremity, especially during movements. These patients, too, will report that "stretching feels good." Just as the previous example, however, we must strengthen the UT in these patients, with proper positioning as explained earlier. The purpose of this post was to make us all more aware and pay specific attention to the scapulohumeral positioning both statically and dynamically in order to determine the true impairment that lies with the UT, or if there even is one at all. A starting point we like to use is assessing the medial side of the scapula at rest to determine if the resting position is upward or downward rotation. That should be followed up with a comparison of the superior angle of the scapula to the acromion as well to aid in confirmation. This positioning should then be tracked during flexion/abduction of the humerus. This is just one muscle's impact on the upper quarter, but as you can tell, it is a significant one. For more information on the topic, it is recommended you review the references listed below. References:
Kendall FP, McCreary EK, Provance PG, Rodgers MM, & Romani WA. Muscles Testing and Function with Posture and Pain. 5th edition. Baltimore, MD: Lippincott Williams & Wilkins, 2005. 326. Print. Sahrmann, SA. Diagnosis and Treatment of Movement Impairment Syndromes. St. Louis, MO: Mosby, 2002. 206-208. Print.
8 Comments
Scott
3/3/2014 02:32:19 am
Great post. One exercise for the UT would be to hold a dumbbell (or just arm weight if sufficient) and flex your shoulder 180 deg, then shrug from there. You're increased the upward rotation, but you also decrease the relative weight of the arm and reliance on front deltoids from the 90 deg flexed position you noted.
Jason
4/8/2014 05:42:47 am
This can actually be an excellent position for strengthening the serratus anterior in a more functional position as well by having them use the "plus" movement (as in push up plus) instead of a shrug if you needed more input from serratus. Having them hold the "plus" while lifting the arms off the wall allows you to hit the lower trap as well - also an upward rotator.
steve karas
3/3/2014 10:57:11 am
Some issues:
Hi Steve,
Steve K
3/3/2014 09:47:30 pm
OK, so not "functioning properly." So other than the lateral scapular glide test (I think that is the name) how do we quantify that? Is it strictly subjective? The best way to "quantify" it would be to assess the scapular positioning both statically and dynamically. Other than that, I recommend identification of the movement impairment syndrome per Sahrmann. Personally, I am relying less and less on special tests. I have found them to be useful in limited situations. For example, there is a very good cluster for identifying those with subacromial impingement. While this is useful, I honestly have seen only one case of true subacromial impingement in the last 6 months. I much more frequently see anterior impingement/anterior humeral glide syndrome, which also tests positive frequently on impingement tests but does not respond to the same treatment. As physical therapists, we are movement specialists. A dysfunction may only appear with these sorts of observational assessments and not with any specific special test. That being said, I believe there is a test where you assist the scapula in elevation and upward rotation. A decrease in symptoms may indicate lack of sufficient upward rotation/elevation. Additionally, Sahrmann recommends that if a patient has pain just sitting there or with cervical movement and it is decreased with passive elevation and support of the upper extremities (taking tension off the scapular elevators), that may also indicate insufficiency. I hope this helps!
Chris
3/27/2014 01:12:57 am
A lot of the research by Kibler discusses more current ways to "qualify" scapular dyskinesis. The article published by BMJ - Clinical implications of scapular dyskinesis in shoulder injury: the 2013 consensus statement from the ‘scapular summit’ - talks quite a bit about using dynamic scapular dyskinesis tests (SDTs). I'm sure many of you have come across this work, but I really enjoyed that article, especially his bit on decreasing our overuse of the word "impingement". Leave a Reply. |

Dr. Brian Schwabe's NEW Book in partner with PaleoHacks!

Learn residency-level content on our
Insider Access pages 

We value quality PT education & CEU's. Click the MedBridge logo below for TSPT savings!Archives
July 2019
Categories
All
|
 RSS Feed
RSS Feed